Lecture
Praxis (from the Greek. Praxis - action) - the ability to perform successive complexes of movements and perform targeted actions according to a plan. When performing complex motor acts, the work of the skeletal muscles should occur in the correct sequence with simultaneous contractions of many muscle groups. Such actions arise in the process of vocational training.
Complicated actions are formed on the basis of kinesthesia - continuously incoming information from proprioceptors when performing any movements. A significant role belongs to the visual analyzer. Speech signaling (oral and written) is particularly important in the training and execution of complex motor acts of a person. Therefore, praxis disorders, primarily related to the pathology of a kinesthetic analyzer, also depend on the impairment of speech functions. On the other hand, for the implementation of the latter requires perfect praxis of speech organs.
Apraxia is characterized by the loss of skills developed in the process of individual experience of complex targeted actions (domestic, industrial, symbolic gestures, etc.) without pronounced signs of central paresis or impaired coordination of movements.
In classical neuralgia, several main types of apraxia are distinguished.
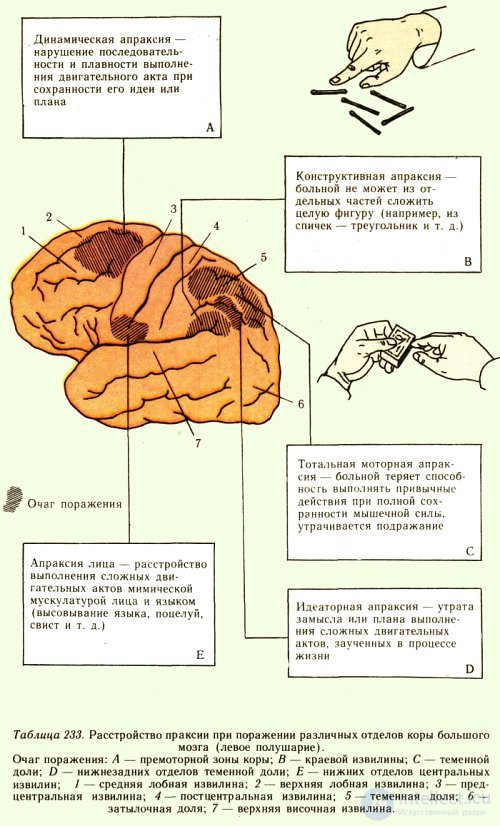
Ideatorial apraxia is caused by the loss of a plan or intention of complex actions, and the sequence of individual movements is disturbed (for example, at the request of showing how to smoke a cigarette, the patient picks up this cigarette on the box, then pulls out a match and stretches it to the mouth). Patients can not perform a number of verbal tasks, especially symbolic gestures (to threaten with a finger, to give a military greeting, etc.), but they are able to repeat, imitate the actions of the investigator. Ideatorial apraxia occurs when the supracarpus gyrus of the parietal lobe of the dominant hemisphere is affected (in right-handers - the left) and always bilateral.
With constructive apraxia, the correct course of action suffers above all; it is difficult for patients to construct a whole of parts, for example, to fold a given geometric shape (a rhombus, square, triangle) out of matches. In this type of apraxia, lesions are more often found in the angular gyrus of the parietal lobe of the dominant hemisphere. Apraxic disorders are also bilateral.
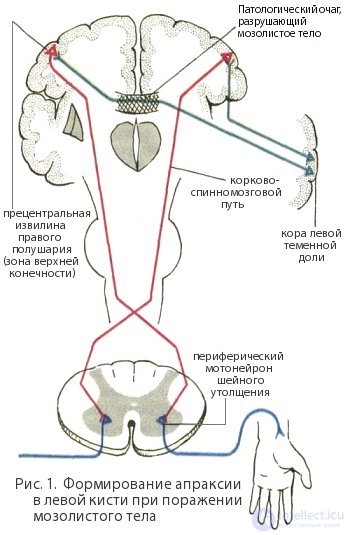
Motor apraxia, or apraxia of the performance of the Dejerine , is characterized by a violation not only of spontaneous actions and actions on the assignment, but also by imitation. It is often unilateral (for example, if the corpus callosum is affected, it can occur only in the left upper extremity) (Fig. 1).
The defeat of the parietal lobe near the postcentral gyrus causes apraxia due to impaired kinesthesia ( afferent, or kinesthetic, apraxia ). The patient can make an arbitrary movement only with constant visual control.
In the foci at the junction of the parietal, temporal and occipital lobes (the zone of the statokinesthetic analyzer), there are disturbances in the spatial correlations when performing complex motor acts ( spatial apraxia ). The patient can not give a straightened hand horizontal, frontal or sagittal position, draw an image oriented in space, get to the desired point. When writing, it makes spatial errors, being unable to correctly correlate parts of complexly constructed letters and showing signs of mirror writing.
With the defeat of the lower parts of the postcentral gyrus of the dominant hemisphere (right-handed - left), oral apraxia develops, usually combined with motor afferent aphasia. The patient cannot find the positions of the speech apparatus, which are necessary for pronouncing the corresponding sounds, sounds similar in articulation are mixed, the letter is broken.
With the defeat of the frontal lobe (zone of efferent systems) there is a disintegration of the skills of complex movements and an action program with a violation of spontaneity and focus ( frontal apraxia ). The patient is prone to ecopraxia (repeats the movements of the investigator) or inert stereotypical movements that he does not correct or notice. Such patients find it difficult to perform atypical programmed actions: for example, when a doctor asks to raise his upper extremity, the patient must lift a second finger, or in response to one knock, raise his right, and in response to two knocks, raise his left upper or lower limb, etc.
For the occurrence of apraxic, as well as aphasic, disorders, the breaking of connections between the cortical parts of the analyzers (especially kinesthetic) and the executive motor systems is of great importance. Therefore, apraxic and aphatic disorders occur with the defeat of not only cortical, but also deep, subcortical parts of the brain, where the fibers of these pathways are more compactly located.
|
STUDY OF GNOSIS AND PRAXIS
|
The study of gnosis and praxis is done with the help of special tasks. Objects that surround the patient are suggested and their recognition by sensory perceptions (visual, auditory, tactile, taste, olfactory) is tested.
Gestures: how to threaten with a finger, how to give a military salute, send a kiss and others. Imitation of the actions of the doctor.
A study of the ability to produce simple arithmetic in mind and in writing.
Performing tasks on the design of figures (folding matches, cubes).
The study of speech, gnostic and praxical functions requires patience from the patient and the doctor. With fatigue of the patient must take breaks for rest.
Praxis is the ability to perform successive complexes of conscious voluntary movements and to perform targeted actions according to a plan developed by individual practice.
Apraksin - is characterized by the loss of skills developed in the process of individual experience, complex targeted actions (household, production, symbolic gestures, etc.) without marked signs of central paresis or impaired coordination of movements. Depending on the localization of the lesion, there are several types of apraxia.
Kinetic praxis. Motor (kinetic, efferent) apraxia is manifested by a violation of sequential switching of movements and a disorder in the formation of motor links that form the basis of motor skills. Characterized by a disorder of smoothness of movements, “sticking” on separate fragments of movements and actions (perseveration). It is observed in the lesion in the lower portions of the premotor region of the frontal lobe of the left (right-handed) hemisphere (with a defeat of the precentral gyrus, central paresis or paralysis develops, in which it is impossible to reveal apraxia).
We ask the patient to perform the “fist — edge — palm” test in a certain sequence: first, you need to hit the surface of the table with the fist, then with the edge of the palm, then with the palm with the fingers straightened. Please repeat this series of movements at a fairly fast pace. A patient with a lesion in the premotor region of the frontal lobe is having difficulty with
performance of such a task (go astray from a sequence of movements, cannot perform a task at a fast pace).
Kinesthetic praxis. Ideomotor (kinesthetic, afferent) apraxia occurs when the lower parietal lobe is damaged in the region of the superior marginal gyrus, which belongs to the secondary fields of the cortex of the kinesthetic analyzer. At the same time, the hand does not receive afferent feedback signals and is not able to perform subtle movements (however, the focus in the area of the primary fields of the postcentral gyrus causes a gross sensitivity disorder and afferent paresis, which completely loses the ability to control the opposite hand, which is not attributed to apraxia) .
Apraxia manifests itself in the occurrence of disorders of thin differentiated movements on the side opposite to the lesion, when the hand cannot assume the posture necessary to perform a voluntary movement, adapt to the nature of the object with which the given manipulations are performed (the hand-shovel phenomenon). Characterized by the search for the necessary posture and error, especially in the absence of visual control.
Kinesthetic apraxia is detected when performing simple movements. This type of apraxia is manifested both in actions with real objects and in imitation of these actions.
Patient’s request:
- stick out tongue,
- whistle
- show how to light a match,
- show how water is poured into a glass,
- show how to use a hammer,
- show how to hold the pen to write with it,
- dial the phone number,
- comb your hair with a comb,
- we ask the patient to close his eyes, fold his fingers into some simple figure (for example, a “goat”), then destroy the figure and ask the patient to restore it himself.
Spatial praxis. Constructive (spatial apraxia, apractognosia) apraxia is manifested as a violation of coordination of joint hand movements, difficulty in performing spatially oriented actions (it is difficult to make a bed, get dressed, etc.). There is no clear difference when performing movements with open and closed eyes. This type of disorder also includes constructive apraxia, manifested in the difficulty of constructing a whole from individual elements.
Spatial apraxia occurs when the focus is localized in the junction zone of the parietal, temporal, and occipital regions (in the zone of the angular gyrus of the parietal lobe) of the left cortex (right-handed) or both hemispheres of the brain. With the defeat of this zone, the synthesis of visual, vestibular and skin-kinesthetic information is disturbed and the analysis of the coordinates of the action worsens.
Tests that reveal constructive apraxia consist in copying geometric figures, in the image of the watch face with the arrangement of numbers and hands, in the construction of cubes.
Patient’s request:
draw a three-dimensional geometric shape (for example, a cube), draw a geometric shape,
draw a circle and arrange the numbers in it as on the watch face; if the patient has coped with this task, ask them to arrange the arrows so that they show a specific time (for example, "a quarter to four"). Regulatory praxis. Regulatory ("pre-frontal", ideological) apraxia includes violations of the arbitrary regulation of activity directly related to the motor sphere. Regulatory apraxia manifests itself in a violation of the implementation of complex movements, including the execution of a series of simple actions, although each of these simple actions can be performed individually by the patient correctly. The ability to imitate is also preserved (the patient can repeat the actions of the doctor). However, the patient cannot draw up a plan of successive steps necessary to perform a complex action, and cannot control its implementation. The greatest difficulty is the imitation of actions with missing items. For example, it is difficult for a patient to show how to stir sugar in a glass with tea, how to use a hammer, comb, etc., while all the same automatic actions with real objects are performed correctly. Starting to perform the action, the patient switches to random operations, getting stuck on fragments of the started activity. Characterized by ecopraxia, perseveration and stereotypy. Patients are also distinguished by excessive impulsive reactions.
Regulatory apraxia occurs when the prefrontal cortex of the frontal lobe of the dominant hemisphere is affected. Patient’s request:
take out a match from a matchbox, light a match, then put it out and put it back into the box, open the tube of toothpaste, squeeze the paste onto the toothbrush, screw the cap on the tube with the paste.

Comments
To leave a comment
Psychophysiology
Terms: Psychophysiology