Lecture
Summary
The article presents the clinical-anatomical and neurophysiological criteria for cognitive disorders in diseases of the brain. The key features of the multifocal evoked potentials associated with the event are presented in early diagnostics, differentiation of the profile of cognitive impairment, the degree of decline in cognitive functions, and objectification of therapeutic tactics of cognitive disintegration.
Keywords
evoked potentials associated with an event, cognitive disorders, memory, dementia.
The problem of cognitive impairment in a variety of neurological, somatoneurological and psychiatric diseases is one of the most pressing in modern neurology. Nevertheless, it is important to understand that cognitive disorders (CR) are only a syndrome that must be understood within the framework of individual nosologies. In some cases, CR may be the only early sign of the disease, the first and / or dominant symptom. Since these disorders in the early stages of the disease are selective, i.e. selectively involving one of the spheres of cognitive activity, patients and their relatives do not fix attention on this, CDs are underestimated by doctors and the first symptoms often go unnoticed. Late diagnosis and lack of therapy significantly worsen the patient's quality of life, reduce adherence to treatment, and lead to disability of the patient.
Despite the different combination of clinical, neurophysiological, neurovisualizing and biochemical markers in the study of the cognitive sphere, the search for more reliable techniques for identifying and evaluating CD and dementia remains relevant. It is usually possible to diagnose a predominant type of CI only in the early stages of a neurodegenerative process. Subsequently, as CR progresses from selective to total, they lose their specificity and it becomes extremely difficult to type the dementia profile according to neurophysiological and neuropsychological examinations. At the same time, early diagnosis and timely therapy of the CR can prolong productive cognitive longevity and / or adapt the patient in society. In this regard, a further search for standardized and clear criteria is needed, which would envisage not only the presence of risk factors or signs of disease, but also, perhaps, revealed a certain nosological profile of cognitive impairment at the pre-demental stage.
Cognitive functions (lat. Cognitio - cognition) - complex integrative processes of processing external information, through which knowledge of the world takes place and interaction with it is provided. This process includes four main interacting components: 1) perception of information, attention; 2) processing and analysis of information (gnosis, praxis, counting, thinking, orientation); 3) memorization and storage of information; 4) exchange of information, construction and implementation of an action program (psychomotor coordination, speech, planning and control of higher mental activity).
CD is spoken in cases where there is a deterioration in one or more of the above areas as compared with the premorbid level, that is, a decrease in the number of intellectual abilities relative to the individual norm for a particular person [34, 108, 111].
There are 3 degrees of KR:
1. Easy degree. Minimal cognitive deficiency - the patient is fully oriented, performs well psychological tests that determine the state of the operational memory, controls his behavior and emotions, easily performs 2-3 complex instructions, but at the same time he has a certain decrease in concentration, mental performance, memorization of new material .
2. Moderate degree. The patient is periodically confused in time and space, there is a moderate decrease in the RAM, when performing two-syllable instructions makes mistakes.
3. A pronounced degree - dementia: there are various degrees of impaired memory and intelligence in combination with different degrees of social maladjustment (Table 1).

According to the anatomical localization, such dementias are distinguished [34, 108]:
- cortical dementia (Alzheimer's disease, lupinal lobar degeneration, alcoholic encephalopathy);
- Subcortical dementia (progressive supranuclear palsy, Huntington's disease, Parkinson's disease, multi-infarction dementia);
- cortical subcortical dementia (Levi's body disease, cortical and basal degeneration, vascular dementia);
- Multifocal dementia (multiple sclerosis, Creutzfeldt-Jakob disease).
The main causes of CD and dementia [34, 57, 108, 111]:
1. Neurodegenerative diseases (Alzheimer's disease, Lewy body dementia, Pick's disease, dementia in Parkinson's disease, corticobasal degeneration, Huntington's chorea, progressive supranuclear palsy, olivopontocerebellar degeneration).
2. Vascular diseases of the brain (consequences of a single stroke in the “strategic” zone, multi- infarction condition, cognitive impairment associated with chronic cerebral ischemia, Binswanger disease).
3. Mixed (vascular-degenerative) cognitive impairment.
4. Neuroinfections, including slowly progressive, and demyelinating diseases: (HIV-associated encephalopathy, spongiform encephalitis (Creutzfeldt-Jakob disease), consequences of acute and subacute encephalitis, multiple sclerosis, multifocal leucoencephalopathy).
5. Consequences of transferred craniocerebral injury.
6. Normotensive (areresorptive) hydrocephalus.
7. New growths.
8. Metabolic disorders and intoxication.
9. Psychiatric disorders.
10. Autoimmune diseases.
11. Medication (antidepressants, anxiolytics, hypnotics, sedatives, anticonvulsants, anticholinergics).
12. Deficiencies.
13. Autism.
Memory is an integral part of the neurocognitive system and differs depending on the duration of storage and use of information, such as semantic organization and anatomorphological formations associated with these processes [8, 27, 59, 67, 90]. The study of memory, which began with the initial conceptual allocation of long-term, short-term memory and neuropsychological studies of patients with focal brain damage, now includes new modern methods, such as positron emission tomography (PET), functional magnetic resonance imaging (fMRV), tractography, evoked potentials associated with event (VPSS), which provided a more advanced classification system mnestic processes [1, 10, 15, 21, 27, 68, 90, 91, 112].
Modal memory impairments apply only to stimuli addressed to a specific analyzer or due to a highly specialized method of information processing. They usually speak of visual, auditory, taste, olfactory, speech, pain, tactile, motor, and musical memory [67, 91].
Depending on the degree of awareness, type of semantic organization and use of information, we distinguish between declarative (explicit) memory - conscious, associative (its subtypes are operational, semantic and episodic memory) and procedural (implicit) memory (classical) reflexes, unconscious automated actions , motor skills [8, 25, 27, 67, 91].
Depending on the duration of information storage, the memory is divided into short-term (operational) and long-term . A variety of RAM is working memory (RP) - this is a decision-making process and a short-term ability to keep the focus of attention and process the flow of information in a quickly retrievable and easily manageable form. Long-term memory is represented by two subtypes - episodic (EP) and semantic memory (SP). Episodic memory is a memory for faces, places, events, objects, verbal and figurative associations. Semantic memory - knowledge of things, concepts, recognition [8, 58, 67, 91, 94].
Below are four memory systems (episodic, semantic, procedural, and working memory) that are important in the clinical diagnosis of mental disorders [27, 59]. Clinicoanatomical differentiation of memory systems is presented in Table. 2
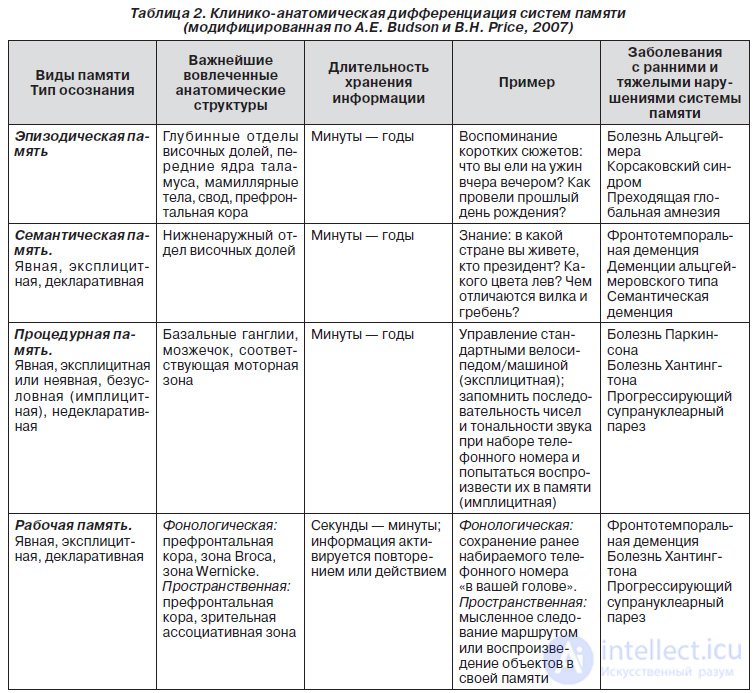
Episodic memory differs from other memory systems in that it gives a person the opportunity to remember past experience, allows one to recall the events that actually took place at a certain point in life. The temporal sequence of episodic memory impairments is described as Ribot's law: recently acquired memories are more vulnerable than memories acquired long ago [58, 91, 94].
Anatomically, the medial divisions of the temporal region of the hemispheres, including the entorhinal cortex and hippocampus (GP), play an important role in addressing memorial marks to certain areas of the cortex [8, 27, 31, 52]. Other critical zones (some of which are related to the circle that Papez described in 1937) include the structures shown in Fig. one.

Along with GP, the frontal cortex plays an important role in maintaining the sequence of events in memory [9, 15–17]. Three groups of neurons can be distinguished in it: some react to the active signal, others retain its trace until the moment when it is necessary to give a behavioral response, and, finally, others include a response [67, 91, 94, 107]. Neurons are discharged sequentially and, as it were, pass the baton from one group to another [22, 24, 52]. Frontal lobes are also important in certain aspects of episodic memory, such as registering, acquiring or encrypting (studying) information, searching for information without a contextual hint, in recalling the source of information, in assessing the temporal sequence and novelty of events [8, 9, 49, 60, 61, 94]. The medial parietal and frontal lobes on the left are involved in the study of words, while these same zones on the right are involved in the study of visual scenes [12, 29, 101, 115]. Memories of distortion and false memories may be due to dysfunction of the frontal lobe, when information is associated with a false context [27].
Alzheimer's disease or Alzheimer's-type dementia debuts with a pronounced progressive impairment of episodic memory [86, 97, 111]. Vascular dementia and other multifocal lesions, such as multiple sclerosis, are characterized by alternating stabilization and stepwise deterioration of episodic memory [108]. In stroke or traumatic brain damage, usually maximal abnormalities are observed in the acute period, and subsequently improve and do not progress. Transient disturbances of episodic memory can occur with concussion, convulsive seizures, transient global amnesia [91].
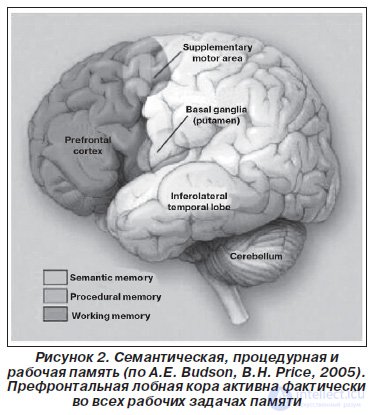
Semantic (semantic) memory (or recognition) is morphologically associated with lower-lateral regions of the parietal lobes, which are involved in semantic tasks associated with contextual processes of naming, forming, classifying and structuring information [50, 113, 117]. However, in the broadest sense, semantic memory is localized in various areas of the cortex that are associated with various types of knowledge [20, 29] (Fig. 2).
For example, a patient with mild dysfunction of semantic memory shows a decrease in the number of words in the semantic category in one minute. Patients with severe disorders have a bilateral semantic deficit: they are not able to name the object when it is described, and also fail to describe the object when it is called [25, 30, 36].
Alzheimer's disease is also a common cause of semantic memory impairment, but its impairment is less pronounced than episodic memory impairment [35]. Patients with a temporal variant of frontotemporal dementia (semantic dementia) have a deficiency in all aspects of semantic memory with a relative preservation of episodic memory [13, 63]. Other semantic memory disorders include any pathology of the infra-lateral region of the parietal lobe, such as traumatic brain injury, stroke, surgical damage, encephalitis, and tumors [29, 96].
Procedural memory is the ability to master behavioral and cognitive skills, algorithms and transfer them to an automatic, unconscious level. The brain regions involved in procedural memory include the motor cortex, the basal ganglia, and the cerebellum [27, 52, 67, 91]. Most often, procedural memory suffers from Parkinson's disease and other disorders affecting the function of the basal ganglia and the cerebellum, such as Huntington's disease, olivopontocerebellar atrophy, strokes and tumors in these areas [14, 28, 43, 44]. The destruction of procedural memory is suspected when there is any loss of previously obtained or significant difficulty in mastering new skills.
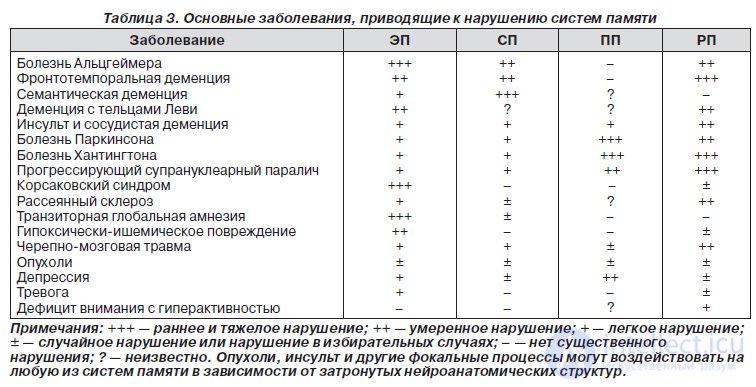
Working memory is a kind of operative memory — a mental process that reflects the ability to concentrate, keep in focus, process and manipulate a certain flow of information in our mind [24, 60, 110]. This is a super-operative memory, which plays a role in everyday behavior and decision making. Working memory is divided into phonological and spatial [8, 27, 67, 91]. However, despite the type of information processed and the complexity of the task, the frontal cortex of both hemispheres is always activated initially, and then, depending on the specifics of the task, other cortical (parietal, occipital) and subcortical zones are included in the neural network [30, 32, 90, 91,] . For example, occipital subordination in visual memory tasks. The left hemisphere is more actively involved in phonological tasks, and the right one is more active in solving spatial problems of working memory [9, 16, 17, 66]. An isolated disturbance of the processes of directed attention, the lack of an adequate response, impulsiveness or slowness of reactions, rapid fatigability under mental loads indicate selective CD with the involvement of working memory [16, 22, 49]. These symptoms are observed with any impairment of the regulatory functions of the frontal cortex, in particular with attention-deficit hyperactivity syndrome [19, 112]. Working memory is closely associated with episodic memory and also worsens in degenerative diseases [31, 107], when the subcortical and lobonetemennye regions are involved in the neural network (Alzheimer's disease, frontotemporal dementia, vascular dementia, Parkinson's disease, multiple sclerosis, strokes, tumors, skull-brain trauma ) (tab. 3).
From the point of view of inter-hemispheric asymmetry , the following memory phenomena were discovered: 1) with direct memorization and reproduction (cognitive novelty), the right hemisphere is primarily involved in mnestic activity, and with delayed reproduction (cognitive routine) - left; 2) with left-sided brain damage, direct reproduction of the material is more intact than with right-sided [17, 21, 22, 49, 52, 60]. The special role played by the frontal lobes and the right hemisphere in the processing of new information and the left hemisphere in the performance of routine actions suggests that the dynamic changes associated with learning are twofold [30]. As we learn, the focus of cognitive control shifts from the right hemisphere to the left and from the frontal ones to the temen-temporal areas of the cortex [30, 49, 113].
Disturbance of neurotransmitter (acetylcholinergic, dopaminergic, noradrenergic, serotonergic) systems occupy a key place in the formation of CD [40, 71]. Degeneration of dopaminergic neurons in the midbrain leads to a decrease in the content of dopamine and its metabolites in the prefrontal cortex, striatum, and the associated zones of the temporal cortex. The decrease in the activity of noradrenergic neurons influences the processing of sensory stimuli in the associative zones of the temporal-occipital cortex and the consolidation of the memory trace [34, 57, 83, 84].
In theoretical, neurophysiological and functional neuroimaging studies, it is common to associate completely specific integrative functions with certain strategic areas of the brain (frontal lobes; temenovascular-occipital regions of the brain; mediobasal divisions of the temporal lobe, hippocampus, anterior and middle sections of the optic tubercles associated with the frontal lobes of the brain; бледный шар, голубое пятно; задненижнебоковой отдел коры и проекция зубчатого ядра полушарий мозжечка) и структурами, функционально с н mi related [8–10, 15, 27]. When solving problems involving figurative, spatial and abstract verbal thinking, the method of mapping cortical connections, fMRI and tractography revealed interaction foci that are typical for different types of thinking, but differ topographically [16, 39, 68, 107, 113]. Focus combines and synthesizes information circulating in various neural networks, on the basis of which a decision is made [39, 49, 68, 89, 107].
In clinical practice, many scales and neuropsychological tests are used to assess cognitive function (Table 4), which require a lot of time on the process of complete patient testing.

Однако отсутствие единой универсальной шкалы, несовершенство тестов, субъективные факторы, влияющие на оценку КР со стороны врача и пациента (формальный подход, индивидуальные возможности и нежелание пациента сотрудничать), приводят к поздней диагностике и несвоевременной терапии КР. Поэтому существует необходимость в оптимальной оценке познавательных функций, объективизации когнитивного статуса, выявлении КР на ранних стадиях заболевания, определении их топической локализации и связи с очаговым процессом головного мозга. Эти данные позволят комплексно определить вовлечение в патологический процесс всего мозга в целом и осмыслить когнитивный статус в рамках отдельного заболевания.
Вызванные потенциалы, связанные с событием (eventrelated potentials), — один из наиболее объективных и динамичных методов мониторинга информационного потока [38, 81]. ВПСС являются неинвазивным и объективным методом, а пациент не может произвольно изменить результат, что часто бывает при психологическом тестировании. Эндогенный электрофизиологический процесс (активность мозга, обусловленная познавательной деятельностью) позволяет оценить интегративные функции практически всех зон, связанных с когнитивными операциями [38]. Нейрофизиологические исследования с применением усреднения ЭЭГ показали, что вызванные потенциалы (ВП) определенной модальности, возникающие в ответ на сенсорную стимуляцию, представляют собой весьма стабильный, хорошо сохраняющий свои формальные и количественные характеристики при повторных исследованиях феномен, который открывает новые перспективы для обследования больных с различными заболеваниями головного мозга [1, 10, 38, 40].
Отклонения в компонентах ВПСС приводят к выводам о природе и локализации мозговой дисфункции, что показано во многих работах [1, 73]. Как правило, эти данные относятся к слуховому и зрительному ВП в исследованиях Р300 при деменциях различной этиологии [82], шизофрении [10, 33], травмах головного мозга [50], интоксикациях [53], нарушении памяти [114]. Изучение ВПСС продемонстрировало возможность определения степени тяжести повреждения, предсказания процесса восстановления после инсульта или травмы мозга [46–48]. Многие авторы подтвердили, что метод ВП является более чувствительным и опосредованным индикатором поражения на ранних стадиях болезни, чем клинические симптомы, и может служить показателем, выявляющим клинически немые зоны поражения [1, 46, 102].
ВПСС, также называемые когнитивными ВП, являются длиннолатентными волнами (более 100 мс). Мозговые структуры и системы, которые генерируют эти компоненты, сложнее ответного сигнала сенсорных образований, в основе которых лежит более короткое время ожидания. Нервные генераторы длиннолатентных познавательных компонентов характеризуются большей специфичностью, поэтому их девиантные амплитуда, время ожидания и распространение на скальпе могут обеспечить полезной диагностической информацией [38].
Классические компоненты ВПСС извлекаются в парадигме, когда подается два типа стимулов: один часто, на который, по инструкции, не следует обращать внимания, а другой значительно реже (20 %) — целевой [40, 58, 73, 80]. В зависимости от модальности сенсорных раздражителей различают зрительные ВП (ЗВПСС) и слуховые ВП (СВПСС). Усредненный сигнал ВПСС представляет собой полифазный комплекс, отдельные компоненты которого имеют определенные амплитудные соотношения и значения пиковой латентности. Последовательность и латентный период (ЛП) компонентов ВПСС отслеживают длительность информационной обработки стимула в миллисекундах в стратегических когнитивных зонах, тогда как их амплитуда указывает на степень вовлечения невральных ресурсов в специфический познавательный процесс [40, 71].
Для большинства ВП известна внутримозговая локализация генераторов каждого из компонентов и их корреляция с данными нейровизуализации (фМРТ, ПЭТ, трактография). Данные фМРИ свидетельствуют, что регистрируемые пики ВПСС четко привязаны к определенному стимулу и фокусируются в соответствующих ему зонах мозга [1, 10, 38]. Это позволяет осуществлять объективную сенсометрию, а также выявлять органические поражения разных отделов соответствующей сенсорной системы по изменениям амплитуды или ЛП отдельных компонентов [26, 56, 87, 92].
Согласно International Society for Clinical Electrophysiology of Vision (ISCEV) standard for clinical visual evoked potentials (2009) различают направленные вверх позитивные волны (P200, РЗ00, Р600) и направленные вниз негативные волны (N100, N200, N400) (рис. 3).

Процесс отбора значимого стимула включает в себя модальноспецифическую сенсорную часть (восприятие), которое связано с физическими параметрами стимула, адресуемого конкретному анализатору, и отражается параметрами ранних компонентов ВПСС с ЛП от 70 до 100 мс.Следующим этапом является первичное опознание и классификация стимулов — N100 ; фиксация новизны стимула при избирательном внимании — MMN [69]; дифференциация, компарация (сличение) стимула с образцом и обновление содержания в памяти ( P200–N200 ) [76]; принятие решения, выбор и подавление действий, контроль результатов, кодирование эмоций и ощущений, пространственный анализ ( P300 ) [10, 81, 84].
Пик Р300 , традиционно называемый когнитивным вызванным потенциалом (КВП), свидетельствует о принятии решения относительно поставленной когнитивной задачи. Пик включает в себя лобные механизмы ориентации и внимания (допаминергический процесс — P3а ) и темпоропариетальный холинергический механизм перераспределения внимания и переработки информации перед ее перемещением из кратковременной в долговременную память — P3b [38, 46, 50, 71].
Обращение к системам памяти и процесс перевода информации из оперативной памяти в долговременную память, определение физических и семантических отличий имеет определенное электрофизиологическое выражение в форме сигнала поздних когнитивных волн от N400 до 700 м с [14, 32, 76]. Около 400 мс — для семантической памяти [96, 106] и 500–700 мс — для эпизодической памяти [30, 41, 58, 66].
Анализ девиаций ЛП и амплитуды сигнала в полной мере позволяет диагностировать топический уровень повреждения головного мозга и выявить мнестические и селективные КР [86, 93].
В комплексном исследовании когнитивных функций нами предложены специальные паттерны [3–5, 38]. Исследование слуховых и зрительных ВПСС проводилось при помощи медицинского компьютерного диагностического комплекса «Експерт» (Tredex, Украина) ТРКО.31940081.0012006 РЭ. Диагностические возможности мультифокальных ВПСС представлены ниже.
Девиация пиков Р100 и N100 — показатель тяжелых КР и задержки когнитивного развития. Они характеризуют раннюю сенсорную обработку информации в первичных корковых центрах. N100 (N1) возникает между 80 мс и 120 мс после предъявления стимула и распространяется над фронтоцентральным регионом скальпа. Его извлекает любой непредвиденный стимул при отсутствии направленного распознавания по предварительному требованию при визуальной, обонятельной, температурной, болевой, вестибулярной, дыхательной и соматосенсорной стимуляции. В случае отсутствия дифференциации данного пика на соответствующий стимул можно сделать вывод, что у пациента присутствует агнозия — нарушено распознавание при сохранной функции анализатора. Для тяжелых КР амплитуда однородновызванного ответа на незначимый стимул фактически превышает ответ на случайный значимый стимул [41].
Топически СВПСС соответствуют 41му, 42му полям по Бродману. Невозможность идентифицировать определенные звуки — стуки, бульканье, звон монет, шелест бумаги и т.п. свидетельствует о простой слуховой агнозии . Невозможность узнать речь, которую больной распознает как набор незнакомых звуков ( слухоречевая агнозия ), развивается при поражении височной области. ЗВПСС соответствуют 17, 18, 19му полям по Бродману. Корковая слепота развивается при тотальном поражении затылочной области. Неспособность подбирать одинаковые цвета или оттенки, а также определять принадлежность того или иного цвета к определенному объекту ( агнозия на цвета ) развивается при поражении затылочной области левого доминантного полушария.
Показатель N100 можно использовать для идентификации поражения слуховой и зрительной систем, когда устные или динамические ответы не могут быть использованы, например в критическом состоянии, коме (слуховые) или апаллическом синдроме и выходе из критического состояния (слуховые и зрительные). Полученные данные являются прогностическими и могут предсказать вероятность восстановления когнитивных функций [38, 40, 46, 48, 114].
The MMN VP (inconsistency negativity) occurs with a typical latency of 150–250 ms after an unexpected stimulus is introduced and reflects the discrepancy between the new stimulus and the idea of a standard stimulus in acoustic or visual sensory memory [10, 76, 80, 116]. Auditory MMN is a negative potential from the frontocentral lead and sources in the auditory cortex of the upper-temporal region and the opercular part of the inferior frontal gyrus on the right (switching attention in response to changes in auditory stimulation) [70]. Visual MMN is an occipital negative potential with sources in the primary visual cortex [69].
The MMN study can verify visual and auditory cortical disorders in patients with coma, in infants and young children, as well as in the absence of patient cooperation or aggravation of symptoms. MMN may be helpful in clarifying the perceptual capabilities of a comatose patient and the prognostic probability of leaving a coma. The presence of MMN, recorded in a comatose state, is 100% predictor of awakening within 12 months. period [46], while the absence of MMN is a predictor of no exit from coma in 84% of cases. The amplitude of MMN correlates with the severity of cognitive dysfunction [33]. The decrease in amplitude serves as an index of cognitive deterioration in the process of aging and in patients with multiple sclerosis [55], with degenerative diseases and the development of dementia [78], observed in patients with schizophrenia [104].
The decrease in the amplitude of MMN is associated with impaired function of NMDA receptors involved in the formation of a memory trace [105], and deterioration of the lobokorkov mechanism in switching attention [23]. MMN can be used to evaluate the effectiveness of dyslexic recovery programs [62].
The lengthening and disturbance of the habituation of the P200 – N200 complex indicates a breach of short-term memory, orientation and attention mechanisms, and a comparison process with known images [22, 76, 102]. The potential of P200 is a kind of selective attention index, which determines a significant stimulus by suppressing insignificant [47]. It was noted that the lengthening of the latency of the P200 peak and the peak interval of the P100 – P200 is characteristic of patients with dementia and in the early stages of Alzheimer's disease [14]. Potential N200 is usually recorded before the motor response, it is associated with the cognitive processes of identifying the stimulus and identifying differences [41, 76, 87, 95]. Complex Р250 – Р270 - final identification of the stimulus, prompt memorization (working memory), comparison of the stimulus with the sample and updating of the content in memory [39, 80]. The prefrontal and dorsolateral premotor cortex is always involved in the task, but in the visual memory tasks it is co-ordinated by the back of the head, and in the auditory tasks the temporal region [41, 56, 76, 85, 87].
The absence of the P200 – N200 complex on the presentation of a spatial pattern indicates spatial spatial agnosia (a disorder in the determination of various parameters of space) and a violation of the topographic orientation , which develops when the dark-occipital region is affected [82, 99].
Deviations of P200 – N200 – P270 to presentation of emotion-like patterns reveal damage to the medial surface of the lower parts of both occipital lobes, ventromedial surface of the temporal lobes and the associated limbic region [25, 28, 51, 92]. In severe cases, if the recognition of familiar faces is impaired, but the objective gnosis is preserved, this may indicate a lesion of the fusiform gyrus ( protopagnosis ). In mild cases, there is a lack of differentiation of non-verbal emotions [25, 26, 64].
Abstract verbal patterns reveal violations of the phonological, syntactic and semantic processes of writing and reading [56, 44, 89, 113]. They include data analysis of the following studies:
- a literal pattern (choose the letter A from the displayed letters and the word with the letter A - 20%). With the defeat of the primary processing area of “visual” speech (reading), alexia is observed. The pathological process in this case is localized in the anterolateral region of the occipital lobe, which is an associative zone for the Wernicke region - the area of speech understanding. This area of the angular gyrus is necessary for understanding the meaning of visually perceptible words. In its absence, a person can perfectly understand speech at the hearing, but does not understand what is written while reading [43];
- grammatical pattern (choose the wrong word - 20%). With a consistent response to the literal pattern, the absence of the P200 – N200 complex for presentation of the grammatical pattern indicates the pathology of the angular gyrus. When this area is destroyed (in the conditions of the Wernicke intact region in the temporal lobe), a person usually normally perceives and understands everything he hears, but the flow of visual information entering the Wernicke region from the visual cortex is basically blocked. Consequently, the patient can see the words and even understand that these are words, but are not able to understand their meaning. This condition is called dyslexia or verbal blindness. Topical localization corresponds to the intraparietal gyrus on the left, the spindle-shaped gyrus and the upper temporal area associated with it [36, 42, 45, 74, 75, 113];
- mathematical pattern (choose an incorrectly solved arithmetic example, the desired number or the required number of subjects - 20%). Acalculia is a violation of the understanding of the structure of a numerical series, difficulties in counting operations themselves, the lack of differentiation of numbers, arithmetic signs, etc. Discalculia is the inability to estimate the number of objects at a glance (that is, without recalculation). This function is associated with the intrapaceous sulcus. In people suffering from this disease, this part of the brain is smaller and not sufficiently active.
Mathematical deviations act as a symptom independent of other disorders of higher mental functions or are secondary. With the defeat of the temporal regions of the cerebral cortex frustrated oral account. With the defeat of the occipital parts are not recognized numbers similar in spelling. With the defeat of the prefrontal divisions, purposeful activity, planning of counting operations and control of their implementation are upset. The lesion of the parietal-occipital-temporal portions of the left hemisphere cortex manifests itself in a violation of the understanding of spatial relationships [72].
VP P300 (P3) - a wave with a positive deviation of about 300 ms - is used as an electrophysiological measure of cognitive function in decision-making processes [66, 80]. Normally, the P300 has a wide topography with a predominance in the frontocentral region, less often in the parietal-central parts with slight interhemispheric asymmetry [54, 76, 81]. Wave P300 consists of two small subcomponents, known as P3a and P3b signals, which are the result of the excitation of postsynaptic potentials generated through glutamatergic networks, where NMDA receptors play a particularly important role [81]. The fMRI data indicate that the P3a and P3b subcomponents are focused in different areas of the brain [112]. The P3a wave has a latency of 220–280 ms and reflects stimulus-controlled frontal mechanisms of orientation and attention — the dopaminergic process in solving the problem, encompasses the lower parietal, cingular, and posterolateral frontal cortex. In some cases, for example, if the deep structures of the parietal-temporal regions are affected, the P3a component can exceed the P3b component in amplitude and can be visualized with a separate wave [18, 98]. The P3b wave corresponds to the main peak of P300, covers the GP, parietal, upper temporal and lateral orbitofrontal cortex and has a higher amplitude over these leads. Wave P3b is associated with many types of higher cortical functions that encrypt an event, including an assessment of the importance of the stimulus, redistribution of attention and processing information before it moves from short-term to long-term memory - a cholinergic mechanism. GABA has an inhibitory effect - reduces the amplitude of the wave and increases the latency time [53]. Acetylcholine is the opposite effect modulator. Cerebral injuries, leading to a deterioration of cholinergic mechanisms of information processing, usually manifest a decrease in the amplitude of the P300 as a whole [38, 50, 71, 88, 100].
The absence or lengthening of the latency of the P300 peak in the presence of previous complexes in the study of all patterns indicates frontal dysfunction. In the case of selective lengthening of the P300, it is possible to judge the disruption of the integrative processes in the cognitive zones corresponding to the pattern shown, for example, the parietal dysfunction in the study of the grammatical pattern (Fig. 3).
Peak N400 is associated with general semantic processes and shows the processing, formation and structuring of information in general, transfer from RAM to long-term, complex consistency of response with memory and semantic plan statements [30, 45, 63, 79, 109]. Topologically recorded over the central-scalp areas of the scalp. In speech understanding models, the N400 peak is often associated with the semantic integration of words into sentence context and linguistic processing [12, 30, 41, 66].
The amplitude N 400 is the basic index of the difficulty of restoring stored knowledge associated with a word and context. This result depends on memorizing the previous contextual task and the lack of semantic and associative understanding [42, 45, 77, 114].
P600 Peak is a linguistically relevant VPSS. P600 can be extracted to the presentation of grammatical errors or syntactic anomalies in ZVPSS (reading) and SVPSS (listening) [42]. Positive peak latency is recorded at about 500–600 ms after the stimulus, mostly from center-parietal and frontal leads. However, this scalp proliferation does not mean that P600 comes from these parts of the brain. The P600 generator is the posterior temporal lobe area. The P600 generator is sensitive to the level of complexity in the proposal and is regarded as syntactic VPSS [42, 48, 65]. For example: problems in the coordination of the verb, adjective, gender, number, which are the cause of the violation of the structure of the phrase “child throw toy”. The study of syntactic and grammatical patterns is important in the diagnosis of damage to subcortical structures. With the defeat of subcortical nuclei P600 is missing [37].
Investigation of memory subsystems: to identify violations of semantic memory, pictures or words are presented that have a literal, verbal or categorical semantic connection with the task. Episodic (associative) memory is checked by demonstrating a pair of drawings or words associated with each other, where the trigger is an associative unrelated pair [75, 103, 114].
We present data and interpretation of complex diagnostics in detecting CU using multifocal auditory and visual CPS.
1. Patient A., 21 years old. Diagnosis: multiple sclerosis, cerebrospinal form, atactic syndrome, lower spastic paraparesis, sensitive disorders, dysfunction of the pelvic organs, reduced vision (EDSS - 4 points).
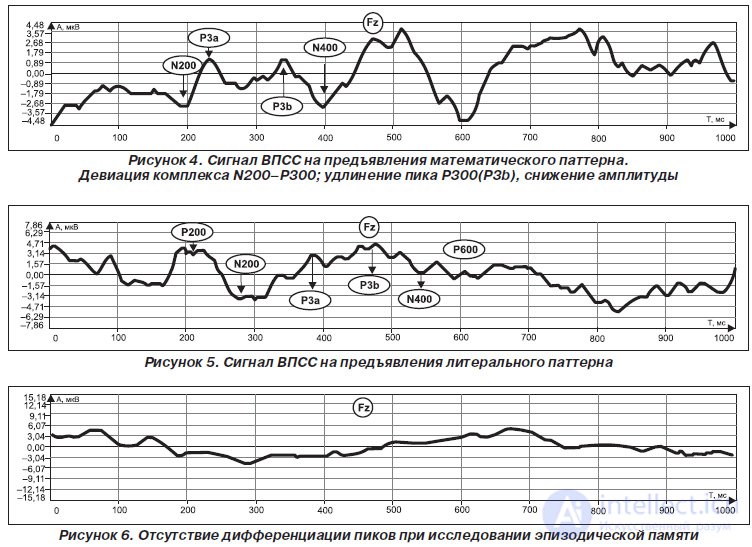
ZVPSS: isolated lengthening of the N200 – P300 complex in the study of the abstract -verbal (literal, grammatical, mathematical) pattern. The data indicate selective cognitive dysfunction with impaired modal-specific working memory (monofunctional type). P300 peak is represented by two visualized waves P3a and P3b. The localization of the focus of impaired cognitive interaction corresponds to the deep structures of the parietal-temporal region with the involvement of associative links with the prefrontal cortex.
Auditory VPSS - without deviations.
A decrease in amplitude indicates a deterioration in the processes of directed attention, a sensory delay in information processing, and a violation of the cholinergic mechanisms of information processing (Fig. 4).
Brain MRI: foci of demyelination in the medulla oblongata on the left (5.5–10 mm), in the pedicle of the left (up to 4.5 mm), in the deep parts of the left temporal area and the white matter of the left parietal area (up to 8 mm)
2. Patient N., 47 years old. Diagnosis: Binswanger disease.
VPSS: lack of differentiation between significant and insignificant stimuli in the study of the spatial, complex abstract verbal pattern and episodic memory.
The P200 – N200 extension is a violation of short-term memory, orientation mechanisms, attention, and a comparison process with known images in the study of literal and auditory patterns.
P300 extension is a violation of information processing and modal-specific working memory in decision-making processes in the study of emotional, literal, and auditory patterns.
N400 elongation, the absence of a positive shift in the late waves is a violation of semantic understanding and associative (episodic) memory.
Absence of Р600 indicates a lesion of subcortical structures.
A pronounced decrease in amplitude, an increase in the P3a – P3b inter- peak interval of the P300 wave indicates a disorder in the processes of orientation and directional attention, and disruption of cholinergic and dopaminergic information processing mechanisms (Fig. 5).
Lengthening the time of sensorimotor reaction.
Evidence suggests multifocal cortex subcortical dementia.
MRI of the brain: the boundary between gray and white matter is not clearly differentiated. In the large hemispheres, many small foci are visualized, located within the white matter and subcortically. In a horizontal section, at the level of the lateral ventricles (T2-weighted image), numerous areas of increased signal intensity are seen in the periventricular white matter, radiant crown and lenticular nucleus. The ventricles and external subarachnoid spaces of the brain are moderately and symmetrically dilated. In the cerebellum - degenerative atrophic changes.
3. Patient N., 79 years old. Diagnosis: Alzheimer's disease.
VPSS: the lack of differentiation of peaks in the study of spatial pattern and episodic memory.
Lack of differentiation between meaningful and insignificant stimuli in the study of a complex abstract-verbal pattern and semantic memory.
The P200 – N200 extension is a violation of short-term memory, orientation mechanisms, attention, and the comparison process in the study of the auditory pattern.
The total decrease in amplitude indicates a breakdown in the processes of orientation and directional attention, a violation of mainly cholinergic mechanisms of information processing (Fig. 6).
Lengthening the time of sensorimotor reaction.
Evidence suggests Alzheimer's type dementia.
Brain MRI: Severe atrophy in the frontal and temporal lobes of the brain, dilation of the temporal horns, reduction in the volume of the hippocampus.
4. Patient F., 14 years old. Diagnosis: dyslexia.
VPSS: lack of differentiation between significant and insignificant stimuli in the study of the grammatical pattern (Fig. 7).
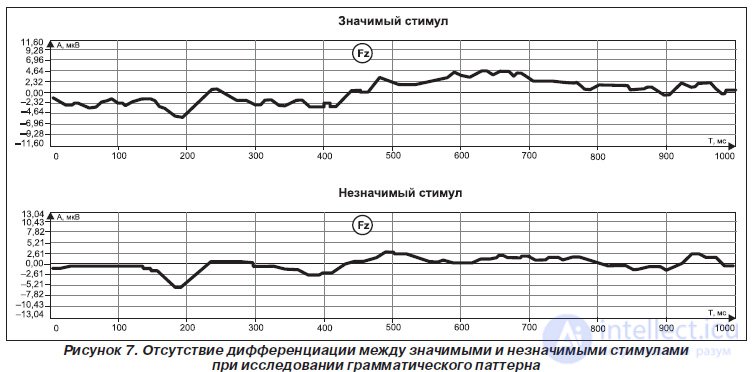
The elongation of the P200 – N200 in the study of the literal pattern is a violation of attention and the process of comparison with known images.
P300 elongation in the study of the literal pattern is a violation of information processing and modal-specific working memory.
Increased amplitude - hyperactivity and impaired attentional processes.
Topical localization corresponds to the intraparietal gyrus on the left, the fusiform gyrus, and the associated upper-temporal area.
No brain pathology was detected on MRI of the brain.
At the moment, for some nosologies, stable parameters of neurophysiological changes in multifocal VPSS have been determined.
Multiple sclerosis:
- total decrease in response amplitude;
- lengthening the time of the sensorimotor reaction;
- selective lengthening of the latency of P300 and N400;
- dissociation of identified MRI foci and profile of cognitive dysfunction;
- predominantly monofunctional type KR.
Post-stroke cognitive impairment:
- in case of focal lesions in the primary associative zones, the complex P200 – N200 was not distinguished, which reflected a violation of the processes of identification and differentiation of stimuli;
- lengthening the latency of the P300 indicates a violation of the RAM and the process of directed attention in the study, addressed to the strategic affected zones of patterns;
- a decrease in amplitude and a change in habituation N400 or the absence of a positive shift in late cognitive waves (P500-700) indicates the difficulty of processing information and reducing the ability to access semantic, episodic memory and procedural memory;
- monofunctional or multifocal type KR.
Alzheimer's type dementia:
- total amplitude decrease with P300 wave latency lengthening;
- visual-spatial agnosia;
- alexia;
- elongation of latency N200 in the study of the auditory pattern;
- lengthening the latency of the N400 peak in episodic and semantic memory patterns;
— амплитуда на новый стимул и фоновый не различаются (амплитуда волны Р300 на новый стимул обратно пропорциональна тяжести апатического синдрома);
— преимущественно амнестический или тотальный тип КР.
Заболевания с поражением подкорковых ядер:
— удлинение времени сенсомоторной реакции;
— отсутствие пика Р600;
— селективное удлинение латентности Р300;
— монофункциональный тип КР.
Аутизм:
— отсутствие дифференциации значимых и незначимых стимулов при исследовании эмоциональнообразного паттерна;
— отсутствие дифференциации поздних пиков при сохраненном и высокоамплитудном комплексе Р200–N200 при исследовании слухового паттерна.
Аффективные расстройства: удлинение латентности компонентов N100 и Р200 при нормальной латентности Р300 и N400.
Выявляемые КР можно разделить на 3 группы:
1. Селективные (монофункциональные) — как правило, связаны с очагом в стратегической когнитивной зоне головного мозга или дисфункцией ассоциативных связей данной зоны.
2. Множественные (мультифокальные) когнитивные нарушения, которые не достигают уровня деменции и характеризуются дисфункцией в нескольких стратегических когнитивных зонах и локальным атрофическим процессом.
3. Тотальные когнитивные нарушения, достигающие уровня деменции и нарушающие социальную адаптацию пациента, обусловлены нейродегенерацией и атрофией головного мозга.
Таким образом, за различиями в нейропсихологическом профиле КР стоит его этиологическая разнородность. Если амнестический вариант КР более четко связан с последующим развитием болезни Альцгеймера и иногда рассматривается как ранняя, «продромальная» фаза этого заболевания, то нозологическая квалификация других вариантов КР встречает значительные затруднения. Дисрегуляторный тип КР, повидимому, наиболее характерен для сосудистой патологии мозга, особенно связанной с поражением мелких мозговых артерий и развитием диффузного поражения перивентрикулярного белого вещества и/или множественных лакунарных очагов. Но аналогичный нейропсихологический профиль может наблюдаться при травмах, ранней фазе алкогольной энцефалопатии, лобновисочной дегенерации, болезни Паркинсона и деменции с тельцами Леви, дегенеративных и демиелинизирующих заболеваниях. Легкий вариант подобного типа с селективными нарушениями характерен и для возрастной когнитивной дисфункции. Комбинированный тип КР при последующем наблюдении может трансформироваться в болезнь Альцгеймера, деменцию с тельцами Леви, но возможен также при цереброваскулярной патологии и особенно при ее комбинации с ранней стадией болезни Альцгеймера. При КР с преобладанием нарушения зрительнопространственных функций в последующем чаще всего происходит трансформация в деменцию с тельцами Леви.
Модифицируя методику исследования ВПСС введением
продолжение следует...
Часть 1 MULTIFOCAL CALLED POTENTIALS, RELATED TO THE EVENT, IN EARLY DIAGNOSTICS OF COGNITIVE DISINTEGRATION
Часть 2 FINDINGS - MULTIFOCAL CALLED POTENTIALS, RELATED TO THE EVENT, IN

Comments
To leave a comment
Psychophysiology
Terms: Psychophysiology