Lecture
It is most reasonable to start studying the phenomena of physicality with an analysis of the subjective intraceptive semantics — the categorical network in whose cells they receive their subjective existence. Since, as we have already noted, intraception is a purely “internal” matter, a convenient procedure for its indirect analysis should be found. The simplest and most obvious way is to compile a dictionary of intraceptive sensations. Its volume, content, age and sex differences, changes in the conditions of various pathologies could help the understanding of specific disorders of bodily perception. The semantic approach is a fairly convenient tool for analyzing the generation and development of intraceptive sensations through the study of the categorical system of their fixation. The choice of this method is connected with the fact that the central psychological mechanism of violations of intraceptive perception is a change in subjective semantics, distortion of intraceptive values and generalizations. Of course, a verbal dictionary cannot exhaustively describe the whole range of intraceptive meanings, many of which are close to “cryptotypes” and do not verbalize well. Nevertheless, these difficulties are quite surmountable.
- An experimental study was conducted in conjunction with O.E. Ephraimus, TS Elderberry, SP. Elshansky.
First, an analysis of the verbalized part of such a dictionary could help to reveal some fundamental regularities. It is completely unnecessary to research the entire dictionary , if the mechanisms of interest to us can be demonstrated on some part of it. The verbalized dictionary is suitable for these purposes, since it is on its basis that complaints are formulated, and it is them, as a system of cultural standards adopted by the subject, correlated with the standard, that mediate the main characteristics of the modality, localization and intensity of bodily sensations.
Secondly, by modeling various actions with this vocabulary, one can try to identify specific individual shades of meanings and meanings that could also help in understanding the breakdowns of bodily perception.
And, finally, the third point: through the verbal dictionary, you can try to build a proper subjective. The idea is that “observations under conditions of“ free instructions ”can help to reveal the structure of the subjective picture of the world (picture of the world for the subject), which reflects his (subject) personality-manipulative features” {Artemieva, 1980, p. 3). If at the same time stable clumps of properties were actualized, this would mean the existence of mechanisms that naturally “pack” the experience of the subject with the world in some special structures. The similarity or difference of the structures of the intraceptive dictionary could also explain the peculiarities of the subjective experience of intraceptive sensations.
The psychosemantic method also provides a very convenient tool for quantifying the various options for impairing the ability to verbalize internal experience. At the same time, unlike the classical methods based on self-assessment, it does not impose high requirements on the reflexive abilities of the subjects, since the very negative result is the object of assessment.
We formulate assumptions in the form of hypotheses:
• The form of the subjective experience of intraceptive sensations, the degree of their development and wealth depends on the subjective experience, assimilation and differentiation of the systems of intraceptual meanings.
• There is a limited number of sustainable ways of structuring intraceptive sensations, which reduces the variety of features used to a finite number of semantic-perceptual invariants.
• Features of the subjective experience of intraceptive sensations and violations of intraceptive perception are associated with
features of intraceptual value systems and changes in the structuring of intraceptive experience.
To achieve the goal - the study of the subjective semantics of intraceptive perception in normal and pathology and testing of advanced hypotheses, the following tasks were set :
• Studying the formation of an intraceptive vocabulary and its structure in healthy subjects.
• Comparative study of the subjective semantics of intraceptive perception in hypochondriac syndromes of various genesis, toxicomania, in patients with real somatic diseases, and in healthy subjects.
In the work, a modification of the psychosemantic method “Classification of sensations” was used (Tkhostov, Efremova, 1989; Efremova, Tkhostov, 1990). It is based on the principle of classification or sorting proposed by G. Miller.
Various modifications of this method are very common in psychosemantics and currently belong to the most adequate methods of structural study of the systemic organization of meanings (Artemyeva, 1980, 1986; Artemyeva, Strelkov, Serkin, 1983; Petrenko, 1983, 1988; Shmelev, 1983; Shmelev, Pohilko, Kozlovskaya-Telnova, 1988).
A close method was proposed by G.A. Arina and I.A. Grape for the differentiation of pain sensations of functional and organic origin (Arina, Vinogradova, 1989).
The stimulus material of the technique was created as follows. First, 1360 words were selected from the frequency dictionary of the Russian language, which could, in principle, describe intraceptive, bodily sensations. Then this set was presented to a group of experts of 25 professional psychologists two times with different instructions:
• “Select words that, in your opinion, are suitable for describing intraceptive sensations.”
• “Select words that, in your opinion, are suitable for describing extraceptual sensations.”
As a result of these assessments, 2 part of the words was selected so that the main patterns could be traced to a smaller
2 The choice of professional psychologists as experts was associated with the need to evaluate the stimulus material by people with a developed ability to self-report, since we were interested in precisely subjective assessments; these experts were preferable to medical experts, distinguished by the "rigidity" of the selection of objective symptoms.
a set of stimuli. The final set includes words that are high-frequency when describing only intraceptive sensations, and words used with equal probability in both cases. If possible, all variants of modalities, intensity, evaluations, main parts of speech, etc. were taken into account.
The final stimulus material of the technique contained 80 definition words, each of which was presented to the subjects on a separate card under a certain number.
The technique included 7 tasks, presented in the following sequence:
I “Select words that you think are suitable for describing intraceptive sensations (if necessary, it was explained that this is an internal, bodily sensation)”;
Ii . “Of the words you have chosen, leave those that describe the sensations you know from your own experience”;
• “Combine" familiar "feelings into groups so that each group has similar, similar in quality";
• “From" familiar "feelings to you, select" painful "”;
• “From" painful "select" dangerous "," health threatening "”;
• "From" painful "select" important, meaningful "."
VII. "From the" painful "choose those that you often experience."
(In the following, when describing the results, the numbering of tasks will be preserved.)
Very important were the I and II instructions, which, in addition to their own value, played the role of preliminary sorts in relation to task III - the free classification of intraceptive signs. Their fulfillment made it possible to exclude the formal approach and, in the course of classification, the subject operated not only with “known” signs, but with signs actually used by him in life.
To process the results of the methodology, a special algorithm was developed, including frequency, correlation, and general variational analysis of results I, II , IV, V, VI, VII tasks and TAXON-analysis of the results of free classification 3.
The TAXON-analysis was subjected to normalized matching matrices constructed after the selection of the most frequent word signs. The advantages of TAXON analysis over other methods of multidimensional scaling are due, first of all, to the lack of
3 The author is grateful to the doctor of physico-mathematical sciences, the head of the laboratory of medical cybernetics of the Oncological Center of the Russian Academy of Medical Sciences T.G. Glazkov for help in mathematical data processing.
requirements for normal distribution of results and ease of interpretation.
He is deprived of many intractable methodological difficulties of factor analysis, more common for psychologists, associated with the choice of orthogonal axes and the identification of factors.
The idea of TAXON-analysis is to build in the Euclidean space of signs-measurements of the spanning tree of minimal dimension. The resulting dendrogram of selected taxa is constructed by successively breaking the most “efficiently” long arcs of the spanning tree, i.e. The features that fall into one taxon have much in common with each other than with the features that fall into other taxa. Theoretically, such a partition can be carried out before the separation of each dimension, but its level of meaningfulness depends on the possibilities of a meaningful interpretation of the resulting groups and the order in which the ruptured arcs of the original covering tree differ. The introduction of the threshold limit (35%) allows you to select a stable part of the dictionary, and the rationing balances the weights of the words included in it.
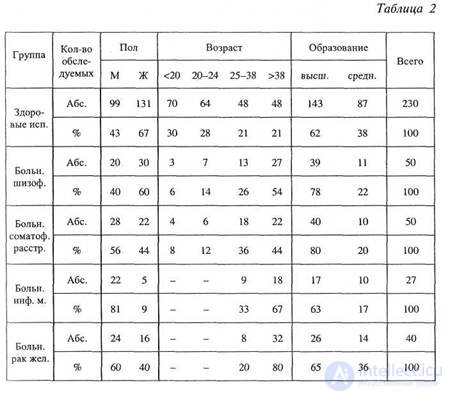
The study was conducted on two groups of patients with hypochondric syndrome in terms of slow-moving (neurosis-like) schizophrenia (schizotypal disorder according to ICD-10, F 21) and somatoform disorder (F 45), two groups of patients with severe somatic diseases: myocardial infarction and stomach cancer and a group of healthy subjects. (In the future, in the figures and diagrams, these groups will correspond to the following numbers: 1 - healthy subjects, 2 - patients with sluggish schizophrenia (schizotypal disorder), 3 - patients with somatoform disorder, 4 - patients with myocardial infarction, 8 - patients with gastric cancer.) In the table 2 shows the demographic indicators of all groups of subjects.
Clinical characteristics of patients with sluggish schizophrenia (schizotypal disorder). Fifty patients with ulcerative slug (neurosis-like) schizophrenia were examined. Disease duration from 0.5 years to 7 years. (The average disease duration is 2.6 years.) The patients were examined at the clinic of the Scientific Center of Mental Health of the Russian Academy of Medical Sciences. For the study, only those patients were selected who, according to the history of the disease, hypochondriacal disorders dominated in the clinical picture of the syndrome and the lack of objective ground for somatic complaints was
confirmed by comprehensive clinical examination. Despite the absence of a real disease, patients presented numerous polymorphic complaints of somatic condition, unpleasant intraceptive sensations, which sometimes had a distinctly senestopathic nature. The diagnosis of schizophrenia was established by a psychiatrist based on dynamic observation.
|
|
Clinical characteristics of patients with somatoform disorder . Fifty patients with somatoform disorder were examined. Disease duration from 0.5 years to 6 years. (The average disease duration is 1.9 years.) Patients were examined on the basis of the Department of Rehabilitation Treatment of Medical Unit No. 21 of the Kalininsky District of Moscow and the clinic of the Scientific Center of Mental Health of the Russian Academy of Medical Sciences. As well as in the examination of patients with schizophrenia, patients were selected who presented numerous complaints of somatic ill-being, not confirmed by clinical examination. The diagnosis of somatoform disorder was established by a psychiatrist.
The choice of such groups was based on the fact that in the symptomatology of these diseases a significant place is occupied by complaints about various intraceptive sensations that do not have real physical grounds. Although in clinical psychiatry one can find a large number of very subtle and detailed differential diagnostic signs that allow them to be separated from real somatic diseases, so far the only indisputable basis for qualifying them as “hypochondriacal” is the impossibility of detection during an instrumental examination of a real organ pathology. Distinction of hypochondriac disorders by their nosological affiliation, in general, is among the most difficult in psychiatry. If you carefully read the relevant sections in textbooks and monographs, it is impossible not to note the extraordinary similarities in the descriptions of these syndromes and purely intuitive, taste preferences in choosing one or another differential diagnostic criteria in the absence of the principles of consistent formalized analysis. Until now, the main criteria for distinguishing them remain the psychiatrist's intuition and long-term dynamic observation.
As reference groups, patients with severe somatic diseases: myocardial infarction and gastric cancer were studied.
Clinical characteristics of patients with myocardial infarction. About 27 patients with myocardial infarction were investigated. This group included patients after a recent myocardial infarction (1.5-2.5 months). The survey was conducted at the base of the department
treatment of NFM number 21 of the Kalininsky district of Moscow. In this experimental group, patients were selected who had not previously submitted complaints of "heart" and had no history of any serious operations and diseases. Often, these patients before a heart attack did not have an outpatient card at the clinic, i.e. they had a heart attack against the backdrop of "practical health."
Clinical characteristics of patients with gastric cancer. Surveyed 40 patients with gastric cancer. Disease duration from 0.5 years to 12 years. (The average disease duration is 2.4 years.) Patients were examined at the base of the clinic of the Oncological Scientific Center of the Russian Academy of Medical Sciences. The group included patients whose post-gastro-resection disorders of varying severity were noted after the prompt treatment of gastric cancer. First of all, it is a dumping syndrome, accompanied by pain and discomfort in the epigastric region, increased fatigue, tachycardia, sweating, increased after eating.
|
|
|
Chapter 7. The study of subjective semantics 165 |
The choice of these particular comparison groups is associated with a very high prevalence of “heart” and “stomach complaints” in hypochondria disorders: “heart attack” and “cancer” are the most frequent diagnoses that hypochondria patients set themselves.
Before the experiment, all patients underwent a complete pathopsychological examination, they underwent a detailed clinical conversation in order to clarify the diagnosis, identify all painful complaints, assess the patient's duration of his illness and its possible causes.
As a control group, 230 healthy subjects participated in the experiment. The main selection criterion in the control group was the absence in the history of the tested severe diseases and operations, as well as chronic diseases in the acute stage.
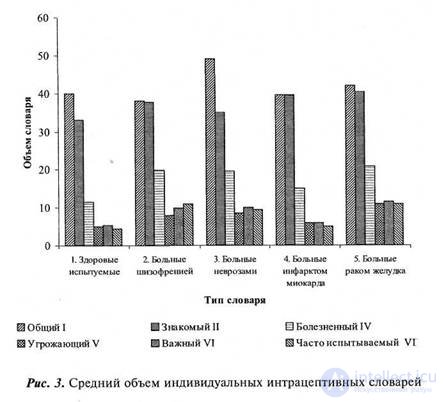
As a result of the experiment, sequential frequency dictionaries were compiled: I - “general dictionary of intraceptive sensations”, II - “familiar from personal experience”, IV - “painful”, V - “threatening”, VI - “important”, VII - “often tested” (numbering is given in accordance with the numbering of tasks). The normal distribution of the volume of dictionaries, confirmed by Chebyshev's criterion, allows further use of parametric criteria for their comparison (Korn and Korn, 1968).
Figure 3 shows a diagram of the average volumes of individual intraceptive dictionaries. As you can see, in healthy subjects, the most extensive is the “common” dictionary, somewhat less than its “familiar” (the differences are not statistically significant), significantly less familiar (p <0.05), the dictionary of painful sensations, the volumes of “dangerous”, “important” and the “often experienced” is about the same and, in turn, significantly less “painful” dictionary.
In patients with schizotypal disorder, the volume of the “common” word is the smallest, while the volume of “familiar” sensations close to it is insignificantly larger than normal in patients with somatoform disorder, and is slightly inferior to the vocabulary volume of patients with real somatic diseases. The dictionary of painful sensations almost doubled (p <0.05) is larger than normal and is the same as in patients with somatoform disorder and stomach cancer.In this group, it is rather interesting to find the nowhere more common ratio of “threatening”, “important” and “often experienced” casualties, each of which is greater than the previous one. If in the other groups these dictionaries practically overlap, then in schizophrenic patients, the principles of sorting are less related.
Significantly more (p <0.05) than in the other groups the volume of the general vocabulary in patients with somatoform disorder. This group of patients is the most, if I may say so, “verbally presented for” and has the best ability to verbalize their body sensations. The same group demonstrates the largest gap between the “common” and “familiar” vocabulary. The latter is practically no different from the same dictionary of healthy subjects. The volume of the painful sensations dictionary is comparable to that of a schizotypal disorder and stomach cancer in patients with a similar disorder.
The distribution of volumes of dictionaries of different types in patients with myocardial infarction is quite remarkable. This group included patients with a serious illness, but little experience of the disease.
neither The most interesting point is the almost complete identity of the “common” and “familiar” dictionaries. This may indicate an exceptional orientation in a situation of acute illness to real-life sensations (a simultaneous increase in the number of “experienced” and less attention to the “familiar” somatic sensations). The volume of “painful”, “dangerous”, “important”, “often experienced” sensations slightly increases and does not reach the volumes of similar dictionaries in other groups of patients. This indicates the need for certain temporal conditions for the formation and expansion of these systems of values, and that at first patients use the categories that they already have to describe the newly created bodily sensations. The first time that happens with these patients- this is an increase in the actual sensations experienced in the framework of the “common” dictionary.
При увеличении опыта болезни реализуется тенденция, хорошо иллюстрирующаяся диаграммой распределения объемов словарей у больных раком желудка. Эти больные с длительным опытом сома тического заболевания и хроническим неблагополучием обладают наибольшими словарями всех типов (за исключением «общего» словаря, где больные соматоформным расстройством недосягаемы). У больных сохраняется ярко проявившаяся у предыдущей группы тенденция уменьшения различий между «знаемыми» и реально испы тываемыми ощущениями.
Итак, подводя промежуточные итоги, можно констатировать, что даже по самому приблизительному и грубому критерию — объему словаря — между выбранными для исследования группами име ются значимые различия. Наиболее информативным и интересным следует считать завышенный объем общего словаря, увеличенную диссоциацию между «общим» и «знакомым» словарем у больных соматоформным расстройством; относительно малый объем «обще го» словаря у больных шизотипическим расстройством и умень шенную диссоциацию «общего» и «знакомого» словарей у больных шизотипическим расстройством и реальными соматическими забо леваниями.
However, quantitative indicators of the volumes of dictionaries can not replace the qualitative analysis of their content. Looking through the layers of the intraceptive sensations of healthy subjects, we can note an interesting phenomenon: along with specific modalitiesьными телесными ощущениями — «тяжесть», «боль», «тошнота»; ощущениями тонуса — «слабость», «усталость», вошли как метафо рические определения типа «страдание», «блаженствовать», так и совершенно очевидные психические состояния — «влечение», «по кой», «тоска», «отчаяние», «возбуждение», «тревога», «предчув ствие» и пр. При этом последние с большей вероятностью включаются в этот словарь, чем конкретные и локализованные «ломота», «зуд», «жжение» и пр. Это прямо подтверждает ранее высказанное теоретическое предположение о том, что объективация телесности проходит не по границе психического и соматического, а по границе управляемости — автономности. Эмоциональные, психические состояния, объективировавшись, став «я-для-себя», расцениваются наравне с объективированным телом, как телесные, составляя, собственно, их костяк. Относя их к телесным, испытуемые хорошо от личают их от конкретно локализованных интрацептивных ощуще ний, но тем не менее выносят вовне сознания, и, не найдя иного места, размещают в границах тела как одновременно и принадле жащего «у?» и им не являющегося. Противопоставляясь «Я», «ис- пытываясь» им как некая упругая реальность, объективированные психические состояния в этом качестве ничем не отличаются от «ис тинных» интрацептивных. При этом таких «квазителесных» ощущений у здоровых людей намного больше, чем органных и буквально интрацептивных, связанных, в основном, с конкретными прояв лениями болезни (чаще всего простудной).
В норме уменьшение «знакомого» словаря по сравнению с «об щим» происходит за счет сокращения конкретных физических симп томов болезненных состояний: «лихорадка», «удушье», «жжение», «зуд», «пронзать», не распространенных в опыте здорового челове ка. Больший объем «общего» словаря по сравнению со «знакомым» говорит об ориентации здоровых испытуемых при построении интрацептивных словарей на усвоенный общественный опыт и о воз можности его отделения от собственного.
Уменьшение «болезненного» словаря по сравнению со «знако мым» связано с исключением из него приятных ощущений («покой», «приятный», «блаженствовать»), признаков отрицательных эмоциональных состояний («отчаяние», «страдание», «подавлен ность»), мучительных ощущений («терзающий», «изнуряющий»), ощущений общего тонуса («вялый», «напряжение», «усталость») и вкусовых ощущений («горький», «вкусный»). В «болезненном» сло варе здоровых испытуемых остаются лишь конкретные физические симптомы («слабость», «дрожь», «жар», «ломота»), которые описы вают наиболее распространенный опыт простудных заболеваний. «Угрожающий», «важный» и «часто испытываемый» словари край-
не малы и составляют несколько устойчивых слов. Все это свиде тельствует о неразработанности словаря болезненных ощущений в норме и испытуемые при их характеристике опираются на знако мые состояния и культурные штампы.
Содержание интрацептивных словарей больных вялотекущей шизофренией (шизотипическим расстройством), на первый взгляд, не очень отличается от словарей здоровых испытуемых. Незначитель ное уменьшение словаря «болезненных» и «часто испытываемых» ощущений по сравнению с «общим» и «знакомым» словарями у больных шизофренией связано с тем, что в нем остаются практи чески все отрицательные («грусть», «тоска», «тревога») и мучитель ные («страдание», «невмоготу», «мучительно») эмоциональные со стояния и ощущения тонуса («вялый», «усталость», «напряжение»), которые здоровые испытуемые не относят к болезненным.
Сравнивая попарно словари интрацептивных ощущений и час тоты выбора каждого признака у больных шизотипическим рас стройством и у здоровых испытуемых, можно видеть, что для ха рактеристики интрацептивных ощущений в целом и описания знакомых ощущений больные шизотипическим расстройством зна чимо чаще используют признаки отрицательных эмоциональных состояний, тогда как такие определения как «удовольствие», «лег кость», «блаженствовать» чаще встречаются в словарях здоровых испытуемых 4 .
Болезненными больные шизотипическим расстройством значимо чаще (р<0,05) называют отчетливо экстрацептивные признаки («мокрый», «стук», «мерцание», «громко»), мучительные ощущения («терзающий», «невмоготу», «изнуряющий»), отрицательные эмо циональные состояния («тревога», «подавленность», «тоска», «отча яние»), ощущения тонуса («усталость», «вялый»), некоторые конк ретные симптомы («давление», «тяжесть», «биение»). Одновременно, некоторые знакомые здоровым людям по субъективному опыту бо лезненные состояния (например: «голод», «отравление») больные используют значимо реже. Последние, как правило, не называются «важными», «угрожающими» и «часто испытываемыми».
К «угрожающим», «важным» и «часто испытываемым» ощуще ниям больные шизотипическим расстройством чаще относят отри цательные эмоциональные состояния («подавленность», «тревога»), ощущения тонуса («усталость», «вялость», «возбуждение»), конк ретные обыденные симптомы («биение», «тяжесть»). При описании наиболее важных ощущений больные также значимо чаще исполь-
4 Это хорошо коррелирует с «агедонизмом» больных шизофренией, отмеченным уже многими исследователями (Поляков, Курек, 1985; Поляков, Курек, Гаранян, 1986; Назаренко, 1990).
зуют экстрацептивные характеристики («вспышка», «мерцание», «темный»), а при описании часто испытываемых ощущений — мучительные признаки («невмоготу», «изнуряющий», «мучительно»).
Характеризуя словари интрацептивных ощущений, очень важ но заметить, что больные шизотипическим расстройством часто используют некоторые слова не в общепринятом значении, что, возможно, становится одним из факторов, на семантическом уров не определяющем появление так называемых «латентных» признаков — характеристике, пронизывающей всю познавательную деятельность этих больных (Поляков, 1974). Так, например, слово «сжиматься» здоровые испытуемые употребляют для описания сер дечных ощущений, больные же — в смысле «весь сжался от напряжения, боли», слово «вспышка» — наоборот, с легкостью исполь зуется для описания ощущений в голове, глазах, а также для характеристики раздражительности («нервная вспышка»). При доступности процессов метафоризации больные шизотипическим рас стройством не обращаются к метафоре, тогда как для здоровых испытуемых это единственная возможность отнесения признака к интрацептивному. Например, слово «всплеск» здоровые испытуе мые используют только в смысле «всплеск эмоций», больные же — для характеристики процессов, происходящих в «больных органах» (например, «всплеск» = «бурлению в желудке»), или описания своих необычных ощущений («как всплеск какой-то внутри»). И еще один пример: больные очень «не любят» слова «бесчувствие», с трудом могут его осмыслить: «Как нет чувств? Чувства есть всег да», — и отбрасывают карточку в сторону. Таким образом, у боль ных шизотипическим расстройством, с одной стороны, происхо дит своеобразное возвращение к буквальному смыслу слова, его родовому корню, а с другой — наблюдается легкость метафориза ции по формальным признакам.
У больных соматоформным расстройством «общий» словарь внешне также похож на словарь здоровых испытуемых, но значи тельно превышает его по объему за счет более частого употребления метафор. Расширение «болезненного» словаря у больных объясняется тем, что в нем остаются ощущения тонуса, отрицательные эмо циональные состояния. Увеличение «важного» словаря происходит за счет привлечения в него ощущений общего недомогания, про студы («жар», «знобить», «плохо»), а «часто испытываемого» слова ря — за счет сохранения в нем ощущений тонуса и тревоги.
При выборе «общих» и «знакомых» ощущений больные соматоформным расстройством значительно чаще используют отрицатель ные эмоциональные состояния («грусть», «подавленность»), ощу щения тонуса («слабость», «вялый»), ощущения в области сердца
(«заныть», «сжиматься», «пронзать»). К «болезненным», «угрожаю щим», «значимым», «часто испытываемым» они значимо чаще отно сят отрицательные эмоциональные состояния («подавленность», «тревога»), сердечные ощущения («заныть», «сжиматься», «уча щаться»), признаки мучительных состояний («невмоготу», «изну ряющий»), ощущения тонуса («вялый», «напряжение»), заурядные телесные ощущения («тяжесть», «онемение», «дрожь»).
Сопоставим различия словарей у больных с ипохондрическими синдромами в рамках соматоформного и шизотипического рас стройств. В «общий» словарь интрацептивных, телесных ощущений больные соматоформным расстройством значимо чаще включают признаки положительных эмоциональных состояний («приятный», «влечение», «удовольствие», «блаженствовать»), отрицательных физических («отравление») и отдельные симптомы («тошнота», «боль»), а больные шизотипическим — экстрацептивные признаки («вспышка», «громко»), а также признаки, которые ни в норме, ни у больных неврозом к болезненным практически никогда не отно сятся («возбуждение», «грусть»). Присутствие подобных «нетра диционных» слов отличает и словари «угрожающих», «важных» и «часто испытываемых» ощущений больных шизотипическим рас стройством. По-видимому, здесь мы также имеем дело с расши рением (или искажением) семантического пространства интрацеп тивных признаков, характерным для интрацептивной семантики больных шизотипическим расстройством.
An interesting fact is that when building “important” and “often experienced” dictionaries, patients with schizotypal disorder significantly more often refer to the word “depression” in patients with somatoform disorder. This may be due to the fact that this symptom is a collective concept for the designation of “special” painful sensations characteristic of this group of patients.
A qualitative analysis of the dictionaries of patients with myocardial infarction shows that an increase in “familiar” sensations is associated with a more active use of specific symptoms related to a previous heart attack. At the same time, these patients are less likely than healthy subjects to use to describe the signs that are marginal assessments of physical (“exhaustion”) or mental (“insensitivity”, “devastation”, “despair”) states, which determines a decrease in the volume of common "dictionary. These patterns are confirmed by a comparative analysis of the frequency of using features in the construction of dictionaries.
In cancer patients, the expansion of all types of dictionaries is associated with the active use of numerous specific
symptoms directly related to the stomach (“burning”, “burn”, “pain”, “ache”) and the general tone sensations associated with the disease (“weakness”, “sluggish”), temperature and local sensations (“aches”, "Shiver"), feelings of the heart ("heartbeat", "increase").
When comparing dictionaries of hypochondriac patients and patients with real somatic diseases, it can be seen that the increase in the volumes of “frequently experienced” dictionaries in hypochondriac patients is caused by a more active use of descriptions of negative emotional states (“anxiety”, “depression”, “depression”) and sensations of tone ( “Weakness”, “tension”, “fatigue”). In addition, patients with schizotypal and somatoform disorders are characterized by significantly rarer use of specific physical symptoms (“burn”, “burning”, “heartbeat”) with more frequent use of signs of negative emotional states (in all types of dictionaries). Dictionaries of patients with hypochondriac syndromes are more metaphorical, “psychologized”, and somatic patients are more real and specific (even the extraceptual signs found in the intraceptive dictionaries of patients with gastric cancer are quite specific: “wet with sweat”, “flicker in the eyes” etc.).
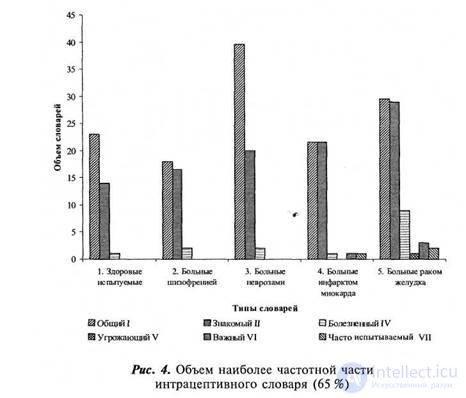
Of interest is the degree of intragroup coordination of elections, which characterizes their homogeneity and consistency with stereotypical use. Figure 4 shows a diagram of the distribution of volumes of the most frequent part of the dictionary - the number of words used by more than 65% of the subjects.
In healthy subjects, the consistency of the “common” vocabulary is significantly higher than the consistency of the really experienced sensations. The smallest intragroup coherence of the “common” vocabulary is demonstrated by patients with schizotypal disorder, which can be considered as a result of the “erosion” of socially developed, stable constructs and the use of latent unstable signs. It is indicative that this symptom manifests itself primarily in the “general” vocabulary, which presumes orientation not only on one's own experience, more or less specific, but on cultural stereotypes. The greatest homogeneity (with the maximum amount) of a “general” vocabulary, indicating a good mastering of standards, is noted in patients with somatoform disorder. Somatic patients demonstrate the consistency of precisely the “tested” sensations, provided by the uniformity and richness of the intraceptive experience, expanding in oncological patients up to pain sensations.
|
|
|
|
In the dynamics of the volume and consistency of intraceptive dictionaries, two trends can be grasped. The first is associated with the development or change of intraception due to the assimilation (or disintegration) of cultural language experience, and the second with the enrichment of categorization through the expansion of one’s own intraceptive experience. The first trend is realized by patients with hypochondriac syndromes, the second by somatic patients.
Deviations from cultural stereotypes and the complication of individual experience have similar external manifestations: reduction of intragroup consistency and leveling up the volumes of “common” and “familiar” dictionaries. This trend is increasing with increasing experience of the disease 5 and is manifested, in particular, in the dynamics of such
5 Since the actual duration of the disease is not always possible to determine exactly, strict formal criteria were chosen: for patients with schizotypal and somatoform disorder, the criterion of the first indicator of stereotype, as the number of words, was never used by the subjects in their triage.
In Figure 5, one can see a clear drop in the consistency of sorts and dictionaries of all types (especially starting with “sick”) in patients with schizotypal disorder and stomach cancer and an increase in concordance of dictionaries in patients with somatoform disorder. The latter demonstrate choral verbal talent and ease of mastering stereotypical medical formulations, which in their intraceptive dictionaries replace the diversity of the living language and the wealth of individual experience.
or repeated (repeated) hospitalization, and for cancer patients - the period elapsed since the operation (more or less than three years). Understanding the known conventionality of such a division, it is possible, nevertheless, to assume that unlike other, no less controversial, it is at least easily verifiable
Although the volume and content of intraceptive dictionaries are quite informative in and of themselves, they do not allow one to judge the basic principles of categorization used by the subjects. The same definition can have different semantic shades and be used in different senses. In addition, it is unlikely that a person uses an unlimited number of ways to organize their experience. Most likely, the number of such coordinates is finite. This assumption is confirmed by the huge number of works on the psychosemantics of extraception, and there is no reason not to assume the possibility of identifying a finite number of coordinates in the intraceptual semantics ( Osgood et al., 1957; Leontyev AA, 1969; Artemyeva, 1980; Petrenko, 1983; Shmelev, 1983).
To solve the problem of identifying such an invariant, a special experiment was conducted on the “free” classification of sensations, which allowed to catch the most interesting moment — the acceptance by the subjects of an individual strategy of counter structuring of perceived stimulation. After the selection of “familiar” intraceptive sensations, the subject was asked under the conditions of a “deaf” instruction to combine the selected words-signs by similarity: “what suits what”, “combine similar sensations” (III instruction). After rationing the similarity matrix, a taxon tree was built.
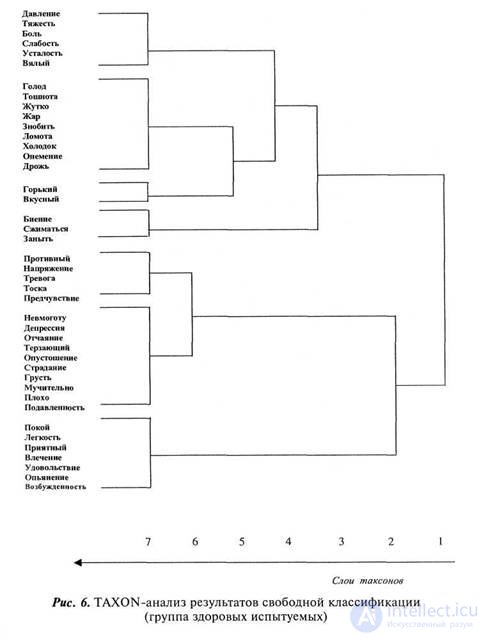
Consider the structure of the taxon tree of intraceptive sensations in healthy subjects (Fig. 6). The primary division at the level of the 2nd layer of the dictionary is divided into two approximately equal groups. The first group includes specific bodily defined sensations, and the second group includes metaphoric and more likely mental, intraceptively experienced emotional states than actually physical ones.
The second division of the taxon tree occurs precisely in this group of “mental states”, which fall into two groups: pleasant and unpleasant. The group of unpleasant (larger) includes metaphorical, emotional and evaluative definitions of the general state. The group of unpleasant sensations persists until the 7th layer, where it is divided into the unpleasant, disturbing, and very unpleasant, painful. From the block of somatic sensations at the level of the 4th layer, a group is distinguished, which includes sensations that can be characterized as sensations in
|
|
Chapter 7. The study of subjective semantics 175
|
|
176 Part 2. Experimental studies
areas of the heart: "beating", "shrink", "zanyt". The remaining group breaks down into feelings of general tone ("pressure", "heaviness", "pain", "weakness", "fatigue", "sluggish") and a group from which later taste and sensations associated with fever or poisoning are distinguished ("Nausea", "fever", "shiver", "chill", "shiver"). The structure of somatic sensations is logical and completely understandable. Actually, intraceptive sensations are not sufficiently objectified and poorly reflected by healthy subjects, they contain the most familiar, frequently used categories: taste definitions, general tone, fever and poisoning. The allocation of cardiac sensations can be explained by the fact that these are the most widely known forms of painful sensations, and the heart, along with the gastrointestinal tract, is the most "developed" organ.
The main dividing criterion for mental, emotional states is the sign of emotion: positive or negative, while for physical bodily states it is attribution to individual organs, body parts, analyzers, serving as the main criterion of similarity-difference. Sensations in the area of the head, heart, abdomen, limbs and gustatory are the most mastered in our culture and have separate dictionaries.
The dictionary of negative emotional states is much richer than the dictionary of positive ones: they form a cluster, almost twice as large as positive ones. There are differences in the qualitative composition of these dictionaries: in the dictionary of negative states, metaphors (“emptying”, “tearing”) bear a heavy load, along with verbal nouns; in the dictionary of positive states, mainly noun-definitions (“peace”, “lightness”, “pleasure”) are presented. The load distribution in the construction of an intraceptive dictionary in favor of descriptions of emotional states, the small differentiation of individual organs and body parts, as well as the use of generalized categories and numerous extraceptual definitions indicate the absence of the intraceptive dictionary itself in healthy subjects.
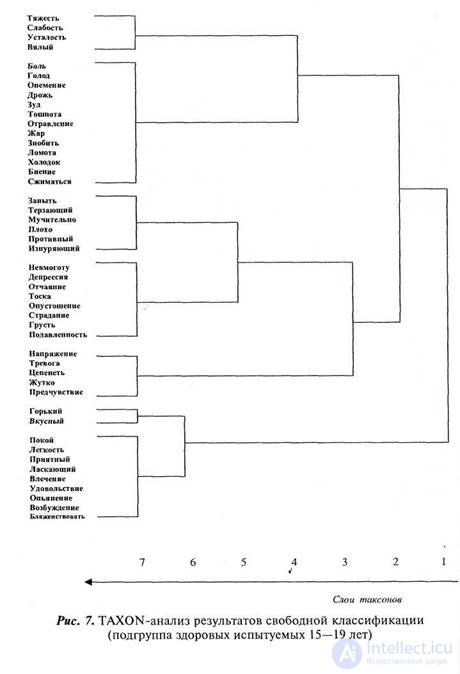
The thesis of uncontrollability, “opacity” as the basic principle of the objectification of corporeality is confirmed by the age dynamics of intraceptive dictionaries. The group of the youngest subjects (15-19 years) is the first to distinguish sensations associated with taste (here the natural objectification is obvious) and erotic excitement (Fig. 7). This, apparently,
|
|
178 Part 2. Experimental studies
one of the first reflective patterns of sustainable intraceptive experience (the transformation of the body from a transparent probe into an object). Actually intraceptive sensations, grouped around the tone and undifferentiated "indisposition" (poisoning, cold) are extremely few. The dictionary is based on negative emotional, anxious and depressive states. Even such somatized sensations as “zanyt” and “exhausting” are understood as mental states, entering with them in one taxon.
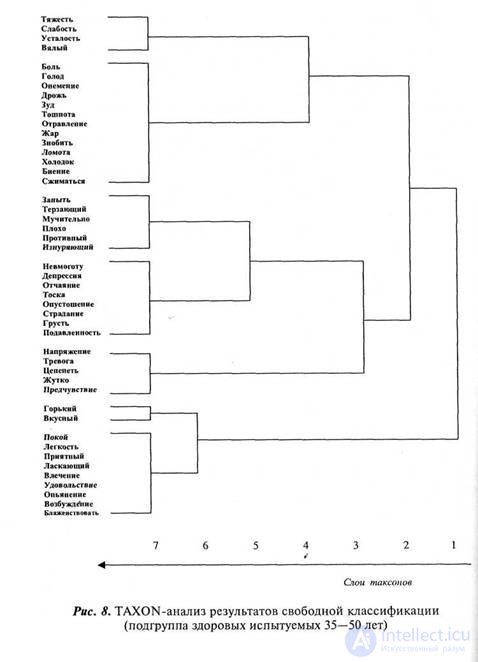
In older age (35-50 years), somatic sensations differentiate significantly better (Fig. 8). There are patterns of sensations in the heart, gastrointestinal tract, temperature, weakness. In the semantic structure, painful experience begins to play an important role: for example, the omission of the tone is no longer simply associated with fatigue, but with painful symptoms. Many definitions contained in the dictionary change their characteristics: the sense of intoxication passes from the category of pleasant to the group of unpleasant, excitement loses its sexual coloring, becoming alarming, and the place of “erotic” objectification is “alcoholic”. The influence of subjective experience on the semantic organization of intraceptive sensations lies in the fact that with age the value of emotionally evaluative categories decreases, the number of specific physical signs increases, the level of objectification of physicality, constructs appear that reflect the experience of disease states, creating preconditions for the development of intraceptive state in norm.
The results of TAXON-analysis of intraceptive sensations in patients become more understandable, taking into account the strategy that they followed. The most important principle was to identify the group of sensations associated with the disease, which included the maximum number of signs selected for the work. At the same time, the usual methods of classification: by modality, localization, emotional tone, etc., were not always maintained. The disease and the sensations associated with it became the center of the classification.
Consider the semantic structure of intraceptive values in patients with schizotypal disorder (Fig. 9). Initially, all intraceptive signs are divided into two main structures: “my disease” (6th and 7th taxa) and “everything else” (taxa from the 1st to the 5th), and the structure “my disease” includes only signs unpleasant mental states, while physical sensations remain outside of it. Further, in the second layer, all
|
|
signs that are not in the “my disease” category are divided into pleasant (7th taxon) and localized painful physical sensations similar to similar groups in healthy subjects (“tone”, “heart”, “general malaise”, “ intoxication is poisoning ”). Pleasant feelings are few and undifferentiated (in one block includes “taste”, “tone” and erotic experiences).
The most interesting phenomenon is that in patients with schizotypal disorder, with an abundance of complaints of somaticпродолжение следует...
Часть 1 PART 2. EXPERIMENTAL RESEARCH Chapter 7. RESEARCH OF SUBJECTIVE SEMANTICS OF INTRACEPTIVE PERCEPTION
Часть 2 7.7. Роль интрацептивной семантики - PART 2. EXPERIMENTAL RESEARCH Chapter



Comments
To leave a comment
The psychology of corporeality
Terms: The psychology of corporeality