Lecture
All our arguments about the possibility of sign-symbolic determination of intraception and the fact that the generation and change of the quality of sensations as subjective phenomena cannot be derived from simple psychophysical relationships will be fundamentally incomplete without a special psychophysical study of bodily sensitivity. The generation of bodily sensations in a situation of mythological mediation - “from the concept” - can be explained, at a minimum, by the action of two reasons (acting, either jointly or in isolation): distortion, in a wide range, of subjective experience, without any changes in sensory sensitivity. the apparatus, or it is precisely these changes in sensitivity arising from factors of extrasensory origin (concentration of attention, attitudes, motivation, past experience, etc.). The solution to this problem is of both theoretical and practical interest.
1 The study was conducted jointly with G.A. Arina, I.V. Moldovana, G.G. Toropinoy, E.O. Screw.
The theoretical value is to clarify the place of psycho-physiological parameters in the construction of bodily sensation not as a natural reflex act, but as a sign-mediated, socialized and transformed in human activity. Although the field of physicality is still regarded as predominantly natural, modern ideas about the nature of sensitivity take into account the possibilities of its extrasensory determination (Zabrodin and Lebedev, 1977; Songaylo, 1962). The development of “subjective psychophysics” is nothing more than a disguised rejection of many prejudices objectivism, which in its consistent realization requires ontological and epistemological exclusion of the subject. In the “subjective psychophysics”, the traditional understanding of the threshold of the sensory system as a boundary separating the continuum of stimuli into sensible and imperceptible and depending only on its physiological qualities, replaces the continuum of stimuli based on the wide variation in thresholds of one and the same person. depending on the conditions of perception and subjective factors. The paradigm of discreteness in understanding the work of the sensory nervous system is replaced by the paradigm of continuity and in experiments on the definition of thresholds, besides its own values, systematic variations and “errors”, habituation or anticipation, and the strategy of signal detection, which take part in the determination of the test response, take full place ( Pennebaker , Watson , 1991).
The practical significance of psychophysical research in patients with functional algic syndromes is related to the fact that it should provide an experimental answer to the question about the place of the functional indicators of the sensory system in the symptom formation of pathological sensations. Without such an answer, a theoretical dispute about what is the primary cause of causing a bodily symptom: the functional state of the corresponding sensory system or the sign system mediating bodily perception is doomed to infinity and psychological speculations on this topic will always be critically perceived by physicians prone to simpler and the usual physiological explanation.
The hypothesis of the study. It was assumed that the influence of sign mediation on sensory and pain bodily sensitivity should be manifested both through a change in thresholds, and through the appearance of typical variations and “errors” of signal perception, the creation of specific strategies. The specificity of intraceptive perception in patients with functional algic syndromes is associated with the peculiarities of their cognitive style, sign mediation, perception strategy, and special types of “errors”.
Objectives of the study. Measurement of sensory and pain thresholds in different conditions of sign mediation, study of the features of the cognitive style, types of strategy and “errors” in the perception of sensory and pain stimuli in healthy subjects, patients with real somatic disease and patients with functional algic syndromes.
The same groups of subjects took part in the experiment as in the experiments on the study of the placebo effect (see Chapter 8, p. 209).
The main research method was the measurement of thresholds of sensory and pain sensitivity (Bardin, 1976). Since it is almost impossible to simulate a true intraceptive sensation in an experimental situation, a measurement of skin sensitivity was used as a model. Understanding the incomplete identity of these forms of sensitivity, we nevertheless believed it possible to establish some fundamental laws which, with certain reservations, could be extrapolated to intraceptive perception.
Theoretically, such a study can be carried out with the help of various stimuli: thermal, Kholodovykh, the method of pressure on the tissue, as well as electrical stimulation {Belyaev, 1986; Kumazawa , Mizunura , Sato , 1987). Technically, the most convenient electrical stimulation. The magnitude of the sensation in this case increases as the strength function of the current within the pain sensation {Zabrodin, Lebedev, 1977; Bowling , 1982).
The electric stimulus was applied using the Stimulus I device, and the current was recorded using a ZIL-1983 FZO digital ampere-volt meter.
Thresholds were measured according to the “boundaries” or “barely perceptible differences” method in the modification called “up-down”. The stimulus was presented in rows descending and ascending in current strength. In the ascending series, the threshold was determined by the signal phenomenon, and in the descending one, the extinction threshold
By the verbal response of the subject, the magnitude of the threshold for the appearance and disappearance of sensation was recorded. The measurement procedure included: 11 samples for measuring sensory sensitivity (9 signal, 1 - “empty”, when the stimulus without warning was not supplied to the expected stereotype time interval, and 1 - “empty”, when the stimulus did not decrease for 30 s) and 7 samples for measuring pain sensitivity (6 - signal and 1 - “empty”, in which the stimulus did not increase after the onset of sensation for 30 s, and after the onset of pain did not decrease for 30 s).
The AC input signal (50 Hz) of a rectangular shape was sequentially (after completing the whole series) fed into two zones — neutral (forearm of the right hand) and relevant for patients with algic syndromes (epigastric region under the right hypochondrium). The study was conducted twice: before and after taking a placebo capsule (Chapter 8, p. 213).
Individual level indicators of sensory and pain thresholds were recorded (average values in signal samples without the first measurement of the threshold of appearance and disappearance threshold), indicators of individual threshold variability (average square deviation).
The mean thresholds and standard deviations of the sensory threshold in a series of pain threshold measurements and gradients of changes in sensory and pain thresholds in pain series (average ratio of the value of the subsequent measurement to the previous one) were calculated separately. Thus, the bodily sensitivity of each subject was characterized by 18 indicators:
• Touch threshold of appearance - SP;
• Touch extinction threshold - SI;
• Pain threshold of appearance - BP;
• Pain threshold of extinction - BI;
• Touch threshold of appearance in the painful series - SP ';
• Touch threshold of extinction in the painful series - SI ';
• The standard deviation of the sensory threshold of appearance - OSB;
• The standard deviation of the sensory disappearance threshold is ICI;
• Standard deviation of the pain threshold of occurrence - BCD;
• The standard deviation of the pain threshold of extinction - OBI;
• The standard deviation of the sensory threshold of appearance in the larger series is OSB ';
• The standard deviation of the sensory threshold of extinction in the pain series is OSI ';
• Gradient of the sensory threshold of occurrence - GPS;
• Gradient threshold of extinction - ГРСИ;
• Gradient pain threshold of onset - PFR;
• Gradient pain threshold of extinction - GrBI;
• Gradient of sensory threshold of appearance in the pain series - HRSP ';
• The gradient of the sensory threshold of extinction in the painful series - ГРСИ '.
These measurements were performed in the neutral (H) and actual (A) zones before the placebo experiment (1) and after (2).
To establish the structure of the internal relations of indicators, the measurement matrix was subjected to TAXON -analysis.
For the analysis of the material, an automated expert system “Pattern Recognition” was used, which made it possible to identify the signs that most informatively separated both groups of subjects and changes in signs (measurements) under the influence of placebo.
Measurement of the effectiveness of external mediation of sensory thresholds
To study the possibilities of external mediation of sensory perception, an experiment was conducted with false feedback. After the first series of measurements and prior to the placebo experiment, a lamp was installed in front of the subject, the flash rate of which correlated with the current applied to the electrode in the current zone.
After 5 installation samples 5 measurements were taken:
• The rate of change of the frequency of the flashing light bulb by 30% exceeded the rate of increase of the current.
• The rate of change of the flashing frequency by 30% lagged behind the rate of increase of the current.
• After the sensation appeared, the frequency of the blinking of the light bulb remained 'stable, and the current strength changed.
• After the sensation appeared, the frequency of the blinking of the light bulb decreased, and the current strength remained stable.
• The change in the flashing frequency was not accompanied by a stimulus.
There were differences in the indicators of the installation series and control measurements. The effectiveness of external mediation was evaluated in ranks (0 — the effect of displacement could not be induced in any sample, 5 — the effect was caused in all samples).
Additional research. Since, on the basis of preliminary experiments, the relationship between the features of intraceptive perception and cognitive style was identified, the level of field dependence was measured for all subjects using G. Vitkin's test.
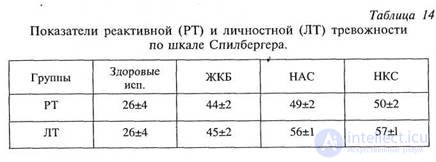
Since there are convincing data in the literature on the effect of anxiety level on the magnitude of sensory and pain thresholds, all subjects measured reactive (RT) and personal (RT) anxiety according to Spilberger's test in a modification of Yu.L. Hanina (1976).
The magnitude of the sensory and pain threshold in our subjects depends on so many simultaneously acting reasons that it is almost impossible to detect any unequivocal logic in its changes. Nevertheless, we will try to single out the main components of these changes and some fundamental laws.
In choosing indicators for discussion, we focused both on their formal (mathematical) information content and on the possibility of meaningful interpretation.
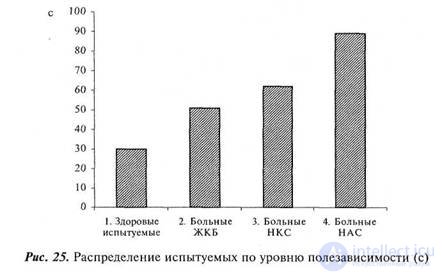
The most informative indicator that distinguishes all groups of patients from healthy subjects is the level of benefit (Fig. 25). As you can see, the most dependent on the field
|
|
|
|
patients with NAS and patients with NCC turned out to be, then patients with ICD followed, and finally, healthy subjects.
The high utility dependence of patients with functional algic syndromes, as the most informative distinguishing feature, well explains the main features of intraceptive perception and symptom formation in this group of patients: reliance on external coordinates, the possibility, within wide limits, of the quality of the stimulus and its subjective experience.
Somewhat surprising for us was the fairly high usefulness of patients with gallstone disease. One may suggest the following explanation of this phenomenon.
First, cholelithiasis itself is one of the psychosomatic diseases and the patients suffering from it differ in a number of peculiar personal qualities, including, apparently, and high initial field dependence.
The second assumption is that this group included patients who were in the preoperative period and differed by a relatively high level of anxiety, comparable to the level of anxiety in patients with functional algic syndromes, which also increased the degree of dependence on the field (Table 14).
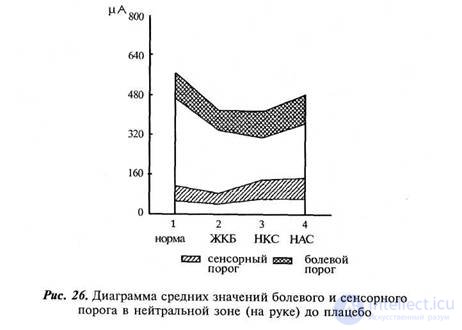
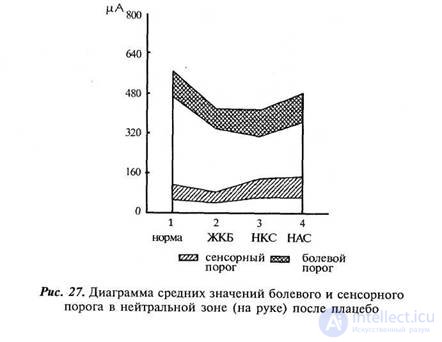
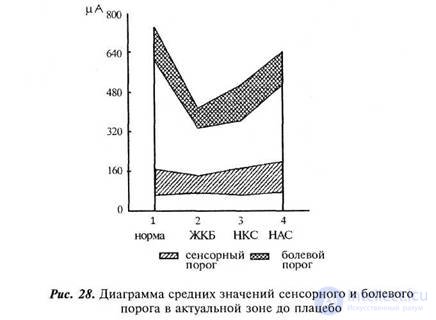
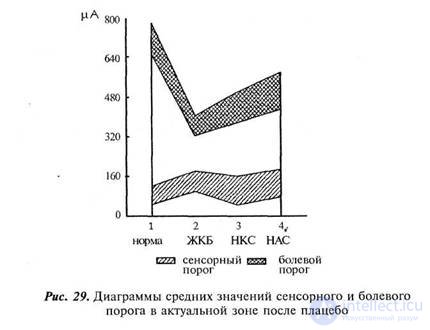
The values of perception thresholds are significantly changed in patients. Figures 26-29 show diagrams of sensory and pain thresholds (appearance and disappearance) in the neutral and actual zones in the first (before placebo) and second (after placebo) series.
We first consider the sensory thresholds and their changes after placebo in the neutral zone. The value of the threshold values on the arm of all groups, except for patients with GIB, is approximately equal, small differences are statistically insignificant. In patients with gallstones, the sensory threshold on the arm is twice as low as in other subjects. Under the influence of placebo, the sensitivity in the neutral zone in healthy subjects increases (p <0.05), whereas in all other groups it decreases, and the difference in sensory porosity increases.
Chapter 10. The study of the influence of sign mediation 243
|
|
|
|
gah becomes statistically significant. At the same time, the difference in the range between the threshold of appearance and the threshold of extinction in all patients, except patients with JCB, increases: the boundaries of sensation after the plate are less clearly defined.
As for the pain thresholds on the arm, their differences are more demonstrative. In all groups of patients, they are significantly lower than in healthy subjects (especially in patients with gallstones, which determine pain sensation most clearly: the difference between the threshold of pain and its disappearance is minimal). Placebo reduces pain threshold in healthy subjects, increasing it in the other groups.
Let us proceed to the analysis of the thresholds of sensory and pain perception in the current zone. The level of the sensory threshold in the area of the hypochondrium and abdomen in all groups of subjects, with the exception of patients with cholelithiasis, in whom it is lowered, is also not significantly different. Placebo significantly lowers the threshold of sensory perception in healthy subjects, insignificantly in patients with NAS and NCC, and raises it in patients with GCB.
Pain thresholds in all groups of patients are lower (p <0.05) than in healthy subjects. The highest sensitivity is observed in patients with gallstones, followed by patients with AUC and NAS. Placebo increases the thresholds for the perception of pain in healthy subjects, does not practically change them in patients with gall bladder and NCC and decreases them in patients with NAS. However, all these changes are statistically insignificant.
Thus, summing up our results, it can be said that all groups of patients have a higher pain (and ICD patients - and sensory) sensitivity than healthy subjects. Theoretically, this should lead to the fact that patients with NAS, NCC and JCB can evaluate pain stimuli of such intensity that for healthy subjects are within the boundaries of normal sensation. In a placebo situation, a systematic increase in sensitivity is observed only in healthy subjects, from which it can be concluded that, although in patients the pain thresholds are initially reduced, the appearance of sensations in the placebo situation cannot be associated with a change in sensitivity (with the exception of healthy subjects who have such hypothesis can be discussed).
During the study of pain sensitivity, we paid attention to a very interesting phenomenon: patients began to talk about what was left of the sensation long before it could be noticed by indirect signs. The feeling was created that some patients called the stimulus painful with an obvious anticipation.
|
|
|
|
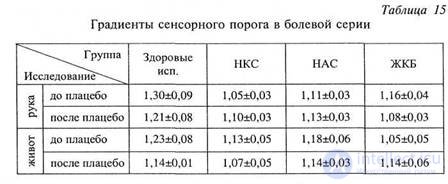
To assess this fact, we used the index of the appearance of the sensory sensation in the painful series. The meaning of this indicator is as follows: after a pain stimulus, the threshold of sensory perception of a sensory stimulus following it increases. The higher the ratio of the subsequent sensory threshold to the previous one, the more reasonably we can speak of physiological pain.
В таблице 15 представлены градиенты сенсорного порога в боле вой серии во всех группах испытуемых.
Поскольку градиенты — величины весьма мало отличающиеся от единицы и средние значения недостаточно показательны, их удобнее анализировать с помощью разбиения на информативные градации (диапазоны измерений, в которых различия сравниваемых групп наиболее выражены).
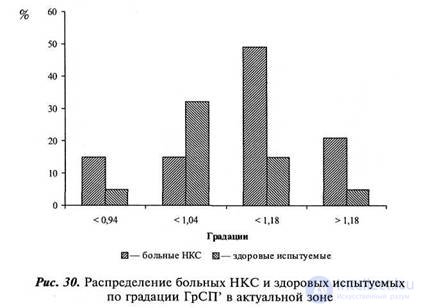
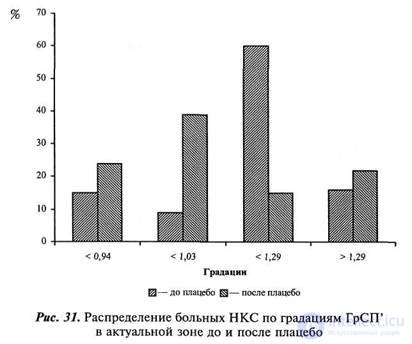
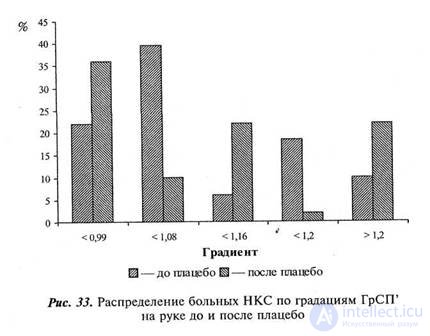
В целом диаграммы распределения количества испытуемых (%) по информативным градациям градиентов сенсорного порога в бо левой серии представлены на рисунках 30—41.
На рисунках 30—33 представлено распределение больных НКС и здоровых испытуемых по градациям градиентов сенсорного порога в болевой серии. Как можно видеть, число больных с низкими (близкими к единице) градиентами значимо выше числа здоровых. В актуальной зоне у 14 % больных градиент даже ниже единицы, что говорит о том, что ни о каком истинно болевом ощущении в этих случаях речи не идет. После плацебо градиенты сенсорных поро гов в болевой серии в актуальной зоне резко падают, а в нейтраль ной (на руке) несколько повышаются.
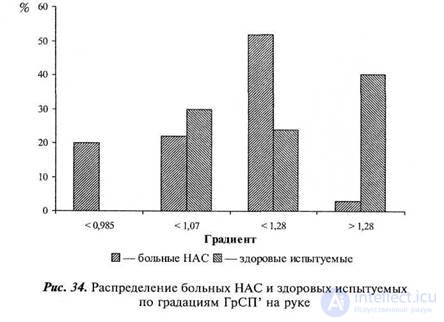
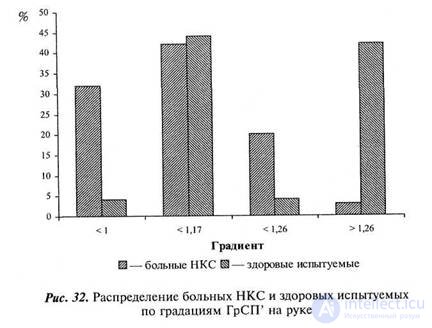
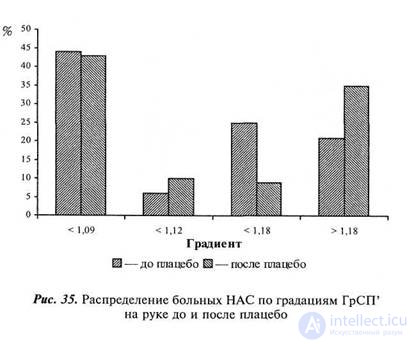
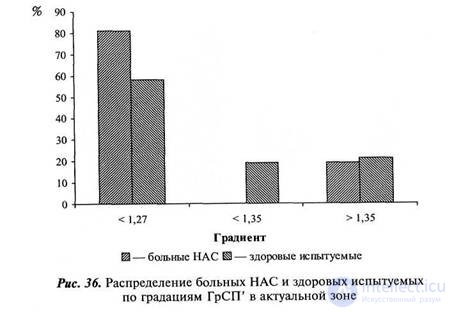
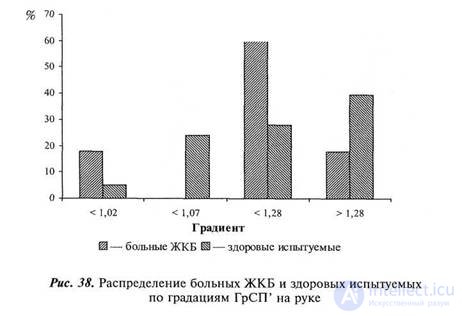
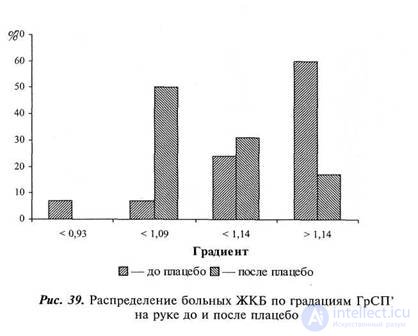
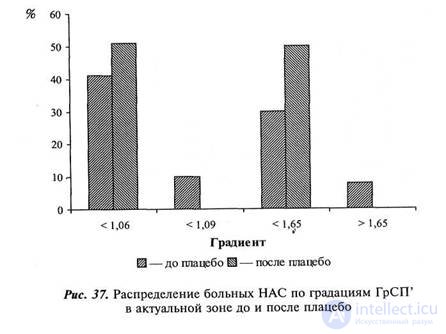
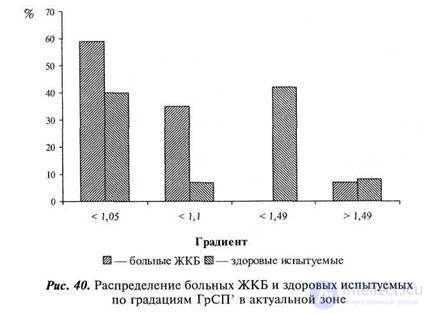
На рисунках 34—41 представлены аналогичные диаграммы для больных НАС и ЖКБ.
Так же как и в случае с больными НКС, у больных НАС гра диенты сенсорного порога в болевой серии значимо ниже, чем в норме и влияние плацебо проявляется в еще большем их уменьше-
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
нии в актуальной зоне и некотором увеличении — в нейтральной. Фиксация внимания приводит к тому, что у более чем 50 % боль ных не происходит никакого увеличения сенсорного порога после восприятия болевого стимула в актуальной зоне.
Несколько иная картина у больных ЖКБ: исходно низкие гра диенты на руке после плацебо еще больше уменьшаются (хотя и остаются, в основном, больше единицы), тогда как в актуальной зоне — увеличиваются, сдвигаясь в сторону физиологической боли.
Для исследования структурной связи между измеряемыми па раметрами был проведен TAXON -анализ матрицы корреляций и построено таксонное дерево сходства 2 .
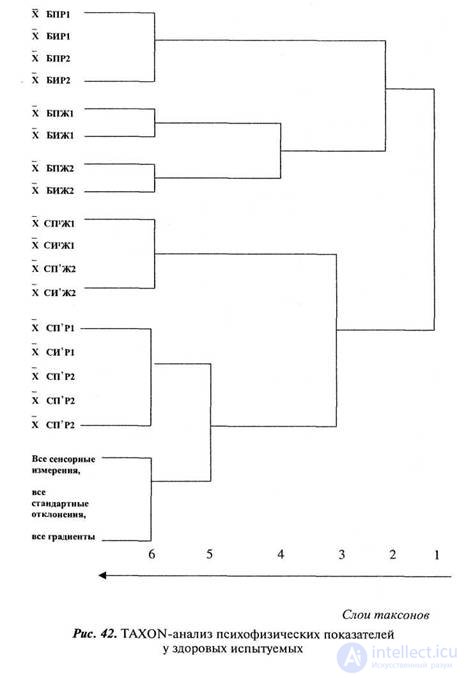
Таксонное дерево измерений у здоровых испытуемых первич ным делением разбивается на два больших класса: в первый входят все болевые пороги, а в другой все остальные измерения. Следую щим делением из болевых порогов выделяется таксон болевых поро гов на руке, сохраняющийся до 6-го слоя, и таксон болевых поро гов на животе, разбивающийся в 4-м слое на болевые пороги в первой (до плацебо) и второй (после плацебо) сериях. Из другой ветви таксонного дерева выделяются на уровне 8-го и 5-го слоев очень интересные таксоны, включающие в себя сенсорные пороги в болевых сериях в актуальной и нейтральной зонах и таксон, вклю чивший в себя все показатели вариативности и градиенты (рис. 42).
Интересны для нас в этой структуре два момента. Во-первых, это то, что болевые ощущения на руке являются наиболее освоен ной и однородной группой ощущений, на которую плацебо не ока зывает существенного влияния. Менее устойчивы, однородны и в большей степени подвержены влиянию плацебо болевые ощущения на животе.
Второй очень важный момент — существование отдельных ста бильных таксонов сенсорных порогов в болевой серии. Они не сме шиваются с простыми сенсорными порогами и их четкое выделе ние отражает факт радикальных изменений сенсорных порогов под влиянием болевого стимула у здоровых испытуемых.
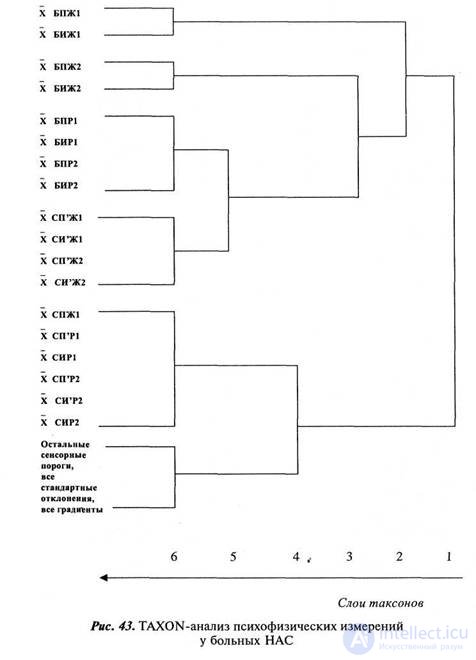
Таксонное дерево измерений у больных НАС строится по дру гой логике (рис. 43). Первичное разбиение происходит не четко по признаку боли (в одну группу с болевыми порогами входят сен сорные пороги в болевой серии на животе). Первыми выделяются таксоны болевых порогов на животе до и после плацебо. Метафо рически выражаясь, можно сказать, что болевые ощущения в об ласти живота у этой группы больных в такой же степени освоены
-2 TAXON -анализ измерений проведен для группы здоровых испытуемых, больных НАС и НКС, группа больных ЖКБ оказалась слишком малочислен ной для получения достоверных результатов.
|
|
и «выделены», как болевые ощущения на руке у здоровых испыту емых. Очень поздно, лишь в 5-м слое происходит дифференциация болевых порогов на руке и сенсорных порогов в болевой серии на животе. Сенсорные пороги в болевой серии на руке не выделяются в самостоятельную группу, а включаются в один таксон с некото рыми другими сенсорными порогами.
Еще более изменена структура таксонного дерева у больных НКС (рис. 44). Первичное деление также не четко проходит по критерию боли. Раньше всего, как и в группе больных НАС, выделяется так сон болевых порогов в области сердца. Он так же освоен и «выде лен», как «рука» у здоровых испытуемых и «живот» у больных НАС.
Наиболее примечательный момент состоит в том, что у боль ных с функциональными алгическими синдромами сенсорные по роги в болевых сериях не разделены с собственно сенсорными порогами. Это, на наш взгляд, дополнительное подтверждение осо бого «болевого поведения» этих больных, при котором стимул, расцениваемый как болевой, никак не влияет на величину сенсор ных порогов в болевой серии, что и делает их неразличимыми с обычными сенсорными порогами.
Обобщая результаты психофизических измерений, можно под вести некоторые предварительные итоги. Пороговые границы боле вых ощущений у больных всех групп значимо ниже, чем у здоровых испытуемых. Причина этого, как нам кажется, заключается не столько в истинном снижении болевых порогов, сколько в особом болевом поведении: как болевое расценивается ощущение такой ин тенсивности, которая не вызывает изменений в сенсорной системе, т.е. это не «психофизиологическая боль», а, скорее, просто «психологическая», и фиксация внимания на теле во время плацебо-экс перимента усиливает эту диссоциацию. Единственный не укладыва ющийся в схему результат — это противоположный тип изменений поведения при восприятии боли у больных желчнокаменной болез нью, у которых происходит замена «психологической» тактики вос приятия болевого сигнала на «психофизиологическую». Возможно это результат специфического отношения больных ЖКБ к самой экспериментальной ситуации измерения болевых порогов. Во время исследования их очень волновало, не сможет ли болевой стимул спровоцировать приступ болезни, они стремились скорее закончить исследование, очень аффективно реагировали на болевой стимул. Ко второй серии эксперимента, убедившись, что процедура измерения безопасна, они несколько успокаивались.
Особый интерес в нашем исследовании представляет анализ типичных ошибок восприятия, систематически встречавшихся во вре мя исследования. Мы выделили 5 типов таких ошибок.
|
|
|
|
• Ложное опознание сигнала: в «пустой» паузе через некоторое время ожидания испытуемый утверждает, что ощущение появилось, в то время как реально стимул не подавался. На наш взгляд, нали чие ошибок такого типа говорит о том, что испытуемый ориенти руется не только на сам сигнал, но и на условия его предъявления, например, временной интервал.
• Ложное исчезновение сигнала: ощущение исчезало, несмотря на неизменившийся характер стимуляции. Ошибки такого типа ин терпретировать значительно сложнее, чем ошибки ложного опозна ния, так как кроме ориентации на условия предъявления стимула возможно влияние физиологической адаптации.
• Ошибки ригидности: у испытуемого после отключения стимула длительное время сохраняется неизменное ощущение.
• Ложное болевое восприятие: без изменения интенсивности сигнала после возникновения ощущения через «ожидаемый» ин тервал времени появляется болевое ощущение. Ошибка, сходная с ложным опознанием сигнала.
• Ложное исчезновение болевого сигнала: без изменения интен сивности стимула болевое ощущение исчезает. Ошибка, сходная с ложным исчезновением сигнала.
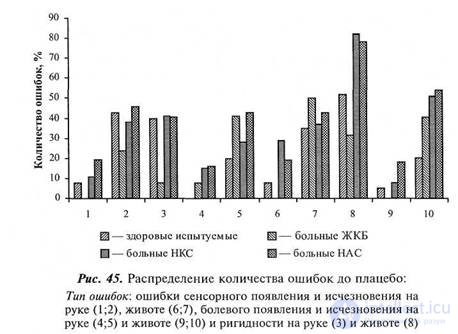
Ошибки отмечались при измерениях сенсорного и болевого порога в актуальной и нейтральной зонах до и после плацебо-эксперимента. На рисунках 45—46 представлены диаграммы количества испытуемых в каждой из экспериментальных групп (%), совершавших ошибки.
У больных функциональными алгическими синдромами количество ложных опознаний и ложных болевых восприятий (как в нейтральной, так и актуальной зонах) значимо выше (р<0,05), чем у здоровых испытуемых и больных ЖКБ. Особенно демонстра тивно это проявляется в ошибках ложного болевого опознания. Плацебо резко увеличивает число ошибок во всех группах. Сам по себе факт ложного болевого опознания, встречающегося после плацебо у 28 % больных НАС и 30 % больных ИКС, является самым силь ным аргументом, доказывающим возможность знакового порожде ния телесных ощущений и его особую облегченность у больных функциональными алгическими синдромами.
Наиболее трудно однозначно трактовать ошибки исчезновения стимула, так как невозможно четко дифференцировать собственно ошибку и естественную физиологическую адаптацию. Число оши бок исчезновения ощущения примерно равно у всех групп испытуемых и равномерно увеличивается после плацебо. Ошибки исчезно вения болевого ощущения, также учащающиеся после плацебо, наиболее редко встречаются у здоровых испытуемых.
Число ошибок ригидности минимально у больных ЖКБ, наибо лее же ригидны ощущения (особенно в актуальной зоне) больных с функциональными алгическими синдромами. Среди больных НКС, например, у 86 % обследованных ощущения сохраняются длительное время после отключения сигнала, изменения ригидности под влия нием плацебо не однозначны и ни в одном случае не значимы.
Обобщая анализ типичных ошибок восприятия, можно отме тить, что больные функциональными синдромами, особенно в усло виях фиксации внимания, склонны к большей ориентации на усло вия предъявления сигнала, чем на качества самого сигнала, частому ложному опознанию сенсорного и болевого стимула («ложным тре вогам») и высокой ригидности возникающих ощущений.
Рассмотрим результаты нашего последнего эксперимента по внешнему опосредствованию сенсорных порогов с помощью лож ной обратной связи. Возможность изменения порогов ощущений оказалась достаточно высока как у здоровых испытуемых (82 %) так и у больных (НКС - 100 %, НАС - 97 %, ЖКБ - 83 %). На рисунке 47 представлена диаграмма средних ранговых значений эффективности внешнего опосредствования. Средний ранговый уро вень у больных функциональными алгическими синдромами более чем вдвое выше, чем у здоровых испытуемых и больных ЖКБ.
Интерпретируя этот феномен в клиническом смысле, можно утверждать, что сенсорная чувствительность больных функциональными алгическими синдромами значимо больше зависит от внешнего опосредствования, чем чувствительность здоровых испы туемых, и эта особая форма «полезависимости», по-видимому, име ет большое значение в формировании симптомов.
Как мы установили, у всех больных (и органическими и функ циональными заболеваниями) снижены пороги болевого восприя тия. При этом фиксация внимания на телесных ощущениях в проце-

дуре плацебо-эксперимента приводит к значимому снижению сен сорных порогов у здоровых испытуемых и практически не отражается на сенсорных порогах у больных. Это позволяет сделать три предположения.
Во-первых, низкие пороги болевых ощущений у больных мо гут обеспечивать более богатую почву для появления телесных ощущений.
Во-вторых, изменения сенсорных порогов у здоровых испыту емых связаны с фиксацией внимания на своем теле. У больных пла цебо может лишь незначительно усилить фиксацию на теле, уже обеспеченную самим заболеванием.
И в-третьих, отсутствие значимых изменений порогов восп риятия после плацебо позволяет достаточно обоснованно предполагать, что появление сенсорных и болевых ощущений в плацебо-эк сперименте (во всяком случае у больных) происходит не из-за простого изменения чувствительности.
Значительно большую роль в порождении телесных ощущений (в симптомообразовании функциональных алгических расстройств) играют другие факторы, выявленные в нашем исследовании: осо бый стереотип болевого поведения, высокая полезависимость и ри гидность телесных ощущений. В стереотипе болевого поведения, ко торому следуют больные, существует значительная диссоциация между психологической оценкой боли и физиологическими след ствиями. Высокая полезависимость, подтвержденная и специаль ными экспериментами и классическими измерениями, связывает качество субъективного переживания ощущения не столько с каче ствами самого стимула, сколько с условиями его предъявления. Высокая же ригидность позволяет возникшему ощущению сохраняться неопределенно долго после исчезновения стимула.
Таким образом, основной причиной функциональных алгических расстройств являются в первую очередь не физиологические изменения организма или сенсорных систем (хотя полностью их отвергать невозможно), а особенности когнитивного стиля, ког нитивной стратегии, через которые реализуется знаково-символическое опосредствование телесной чувствительности.
Я понимаю известную ограниченность полученных результатов в том смысле, что хотя эти рассуждения касались интрацептивных ощущений, реальные измерения проводились на модели кожной чувствительности. Однако это допущение представляется мне доста точно корректным, тем более, что речь идет о достаточно высоких уровнях поведения, которые могут довольно легко экстраполиро ваться на область интрацептивного восприятия.
Неразрешенным остался еще один весьма важный вопрос: что же детерминирует появление стереотипа болевого поведения, высокую полезависимость и ригидность телесного восприятия, каков механизм патогенеза функциональных нарушений чувствительности? Мы не сможем дать на него окончательного ответа, для этого потребуются специальные дополнительные исследования. Задача, стоявшая перед нами, была значительно скромнее: продемонстри ровать на конкретных моделях возможности знакового опосредство вания телесной чувствительности. Тем не менее, некоторые соображения по этому поводу хотелось бы изложить.
Creating a model of a single and universal pathogenetic mechanism for the formation of functional algic disorders, in my opinion, is impossible primarily because the disturbance of bodily sensitivity is a rather heterogeneous aggregate of disorders that have different etiologies and are united only by the similarity of symptoms.
A completely different thing is the modeling of the mechanism for the implementation of a symptom (symptom formation), based on a finite number of general laws of mental activity. In this case, the specificity lies in the choice of certain aspects of this general mechanism, blocking or, on the contrary, facilitating its functioning, in determining this choice. A model of such a symptom realization mechanism could be the idea of a “cognitive style” as a set of specific psychological mechanisms that can be used to analyze the specificity of perceptual determination in various disorders.
So, the degree of field dependence can be both inborn quality, and the acquired characteristic. It may intensify under special conditions, for example, with increased anxiety. Without discussing the rather complex problems of the pathogenesis of changes in the cognitive style, one can safely say that people with a high degree of field dependency and rigidity are at risk of functional disorders of intraceptive perception. This does not mean, of course, that such disorders will necessarily arise, but in situations of stress, emotional distress, or the action of other pathogenic factors, healthy body sensations will be more easily formed in useful and rigid individuals. Anxiety and field addiction can form a vicious circle, when unpleasant bodily sensations arising from situational anxiety, perceived as symptoms of the disease, themselves, secondarily, increase the level of anxiety and lead to a particular stereotype of pain, divorced from the physiological correlates of pain.




Comments
To leave a comment
The psychology of corporeality
Terms: The psychology of corporeality