Lecture
The placebo effect is a very well-known phenomenon in clinical practice. The essence of this phenomenon lies in the fact that this or that effect, which has no real basis for itself and is only symbolically associated with the therapeutic process, causes the subject to feel the changes in his condition. The spread of the placebo effect is so great that, in the opinion of the well-known Soviet therapist B.Ye. At first, his share comes to 60% of the effect of any drug treatment (Quoted in Romenov, 1979). According to other authors, this value almost never drops below 30% ( Beecher , 1959). Nevertheless, despite the prevalence and long history of studying this phenomenon in medicine, its theoretical understanding encounters serious difficulties. Strictly speaking, this phenomenon itself, by its very existence, contradicts the reflex objectivist theory that dominates science
-1 An experimental study was conducted jointly with G.A. Arina, I.V. Moldovan, G.G.Toropina, E.O.Shkrob.
sensations either with the quality of the stimulus or with the properties of the nervous system. In this case, neither one nor the other explanation is suitable, since there is no incentive at all, and one can only assume the influence of a dummy on the state of the nervous system by falling into undisguised idealism.
The only reasonable hypothesis is that taking a placebo pussy pouch fixes attention to intraceptive sensations, leading to sensitization of sensory systems and changes in perception thresholds. Some authors associate the appearance or disappearance of bodily sensations with the influence of anxiety level on sensory thresholds (Medvedev et al., 1984, 1986; Pennebaker , Watson , 1991). However, even in this case, it remains difficult to derive very complex, developed and stable perceptual images from simple sensory changes. The most common explanation comes down to the mechanism of “indirect suggestion,” when “the entire therapeutic effect of an applied pharmacological drug or other remedy is explained by psychological influence” {Roznov, 1979, p. 48). The explanation would be very good if one did not need to understand what constitutes “indirect suggestion” and “psychological influence”.
All these mechanisms undoubtedly take part in the formation of the placebo effect, but none of them can explain it consistently and consistently enough ( Hill et al., 1982; Hilgard , 1971; Melzak, 1981).
In my opinion, the solution to the placebo phenomenon should be sought not only and even not so much in the physiological changes of the sensory systems, but on a psychological level.
As was shown in Chapter 5, the placebo effect can be attributed to a special type of ritual treatment, or, to be consistent, ritual treatment can be viewed as a special case of a placebo effect. The difference between ritual treatment and placebo treatment is only that the expanded ritual that realizes the effect on the causes of the disease in a realistic way is eliminated in the placebo treatment and is only implied. The placebo agent is not any action or substance, but only those that are associated with the myth of the disease and in some way implement the therapeutic effect. Anything can be used as a placebo agent: ritual action, amulet, amulet, physical impact, any material object - the main thing is that it should be associated with the general mythological concept of the disease. In European culture, such an agent most often serves as a placebo tablet as a standard form of “medicine”.
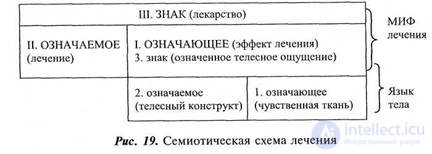
So, we repeat that the only, in my opinion, mandatory condition for acquiring a placebo function by an object or an action is its mythological mediation. The placebo effect is a special case of the implementation of the semiotic treatment scheme. The subject assumes the existence of some “medicine” associated with the myth of the disease and the concepts of treatment and those procedures that implement the “therapeutic effect” (this is not just drinking water, but drinking “holy water”, “ normalization of water balance "or" cleaning slags "). Healing opportunities are virtually contained in the "medicine". From a semiotic point of view, “medicine” is a sign that binds the signified — treatment (use of the medicine) and meaning — the healing effect (the healing effect means that what is being done is treatment). The curative effect as meaning in the mythological system, treatment is nothing more than bodily sensation. The latter, as a marked body sensation, is in itself a sign of body language, combining the signifier (sensory tissue) and the signified (bodily structure).
In the previous part of the work, I said that the secondary meaning, or, as we called it in the traditions of R. Barth, mythologization, distorts the nature of bodily sensation. The bodily meaningful sensation is open in two directions: it is the result of the primary meaning of the sensory fabric and the beginning of the myth — the secondary sign system. I also noted that, being included in the secondary semiotic system, bodily sensations can either change their quality or be generated from above by the myth itself, which needs sensory reinforcement.
The duality of the signifier in the mythological system, which at the same time represents both a hollow form and is sensually filled, allows him to constantly translate the mythological into a concrete-body one. The assimilated, perceived idea of the disease (or the idea of treatment) through the development or selection of elements of the primary semiological system is overgrown with sensory tissue. Possible changes in the sensitivity of the sensory apparatus, if they actually exist, are capable of playing only the auxiliary role of enrichment of the sensory fabric formed into a state construct or modal sensation.
The formation of the myth comes from below, by building on the primary semiological system — the secondary. Learned myth
-2 In this case we are talking about bodily, intraceptive sensations, but without any restrictions the scope of the therapeutic effect can be expanded.
|
|
able to generate its own "reinforcing" reality, finding for the already ready signified the missing meaning. A typical example of this kind is treatment, which can be viewed as the unfolding of a mythological scheme in the opposite direction: from the secondary semiological system (the myth of treatment) to the primary (body language) (Fig. 19).
Since the drug acts as a sign here, regardless of its specific content, it can be replaced by a placebo agent, a ritual or any other subject that, based on the idea of the disease, can play its role. It should be noted that the medical myth is not necessarily decorated in the form of an expanded, comprehended, verbalized and logical construction. As well as the myth of the disease - this is a weakly structured area of assumptions, expectations, prejudices, “cryptotypes”, which is open to constant outside influence.
Psychologically, any treatment is a landmark process, and as such, placebo treatment is no worse and no better than any other. The fact that placebo is a dummy is of no fundamental importance; It is important that, as in the case of a ritual, a person believes in it and fits into the myth he accepts. The fact that placebo treatment is so easily confirmed by bodily sensations depends on completely different reasons - on the particular features of intraceptive perception (difficulties of verification, manipulation, etc.), some of which we have already touched, and others we will try to turn to below.
It is convenient to conduct a study of the effect of a secondary sign on bodily sensations on a placebo effect. It is easy to simulate it under experimental conditions, which make it possible to evaluate the role of factors that influence the shape and intensity of its manifestation in various conditions. For purposes of consistency, the description of the experimental material and the results obtained are more conveniently divided into several blocks.
I unit of research, which will be described in this chapter,
It is devoted to the analysis of the phenomenon of the placebo effect in various groups of subjects, the forms of its manifestation and severity in various experimental conditions.
II block of studies, the results of which will be presented in
Chapter 9 deals with the study of placebo treatment for a long time cut and the analysis of the factors determining its effectiveness.
The III block of studies (Chapter 10) is devoted to the analysis of cognitive
factors involved in the symptom formation of functional algic disorders and the effect of placebo on the sensitivity of sensory systems.
Specific hypotheses, goals and objectives of each unit of research are described in more detail in the respective chapters.
Referring to block I.
Hypothesis of the study: it is assumed that the bodily, intraceptive sensations included in the structure of the placebo effect are assimilated and well-known bodily structures, i.e. primary semiotic system of body language. The placebo effect itself cannot be considered a uniform and stable phenomenon, the form of its manifestation and intensity depends on the type of placebo agent, presentation conditions and the method of inclusion in the secondary semiotic system of the myth.
The objective of the study: to assess the effect of body language and the way in which the placebo agent is incorporated into the secondary semiotic system on the form and intensity of the placebo effect in various groups of subjects.
Patients with functional algic syndromes were selected as the main experimental groups: abdominal and cardiac, with healthy subjects as the control group; comparison groups - patients with gallstone disease. Table 6 shows the distribution of subjects by age and level of education.
Clinical characteristics of patients with neurogenic abdominal syndrome. 48 patients with neurogenic ab-
|
|
dominalgic syndrome (NAS) - F 45.32 - somatoform autonomic dysfunction of the lower part of the gastrointestinal tract. Disease duration from 1 to 25 years (average duration of the disease is 6.9 years). Patients were examined in the clinic of nervous diseases, the department of pathology of the autonomic nervous system, interclinical laboratory of functional diagnostics and the clinic of propedeutics of internal diseases of MMA named after THEM. Sechenov.
Preliminary therapeutic examination of patients with NAS completely excluded organic damage to the organs of the abdominal cavity, small pelvis and vascular system.
Neurological examination data showed the absence of the current organic disease of the nervous system.
In patients for a long time, pain and discomfort of abdominal localization were noted (in 21 people - persistent, in 27 - paroxysmal). By their nature, intraceptive sensations were burning, aching and pulling, gripping or pulsating (most often there was a combination of several sensations).
Associated diseases of the gastrointestinal tract, noted in 10 patients, and gynecological diseases in 15 patients, could not explain the picture of the abdominal syndrome. Despite the absence of any convincing data on organic changes in the abdominal cavity, these patients were repeatedly in various therapeutic and surgical hospitals due to persistent complaints.
Traditionally, abdominal sensations with the exclusion of somatic disease were explained in neurology as manifestations of damage to the peripheral parts of the autonomic nervous system, autonomic ganglia and the solar plexus (Markelov, 1939; Rusetsky, 1959; Chetverikov, Urusmambetov, 1969). Thorough studies of substrate confirmation of such lesions at the microstructural level are still being conducted, but no conclusive evidence of its existence has been obtained, and at present, the concept of neurogenic abdominal syndrome, a heterogeneous clinical phenomenon in which the pathogenesis is dominant, has taken the place of solarium in neurology. psychogenic factors: connection of abdominal attacks with actual psychogenias, conflicts, increased emotional instability and anxiety these patients. This scheme follows the concept of a three-stage formation of psychosomatic diseases: mental disorders - vegetative and endocrine disorders - somatic disorders ( Vein 1971, 1974; Vein, Solov'eva, Kolosova, 1981). Since the idea of the possibility of a pathological sensation without a substrate is unnatural for an objectivistically oriented medical consciousness, the concept of a neurogenic abdominal syndrome can solve the problem by transferring a defect from an area of organic damage (not yet found) to the area of functional disorders of the vegetative nervous system, in a more comprehensible way connected with the reality of the mental.
Clinical characteristics of patients with neurogenic cardiac syndrome. A total of 37 patients with neurogenic cardiac syndrome (AUC) were examined - F 45.30 - somatoform vegetative dysfunction of the heart and cardiovascular system. Disease duration from 2 months to 12 years (average duration of the disease is 3.3 years). Patients were examined in the clinic of nervous diseases, the department of pathology of the autonomic nervous system, interclinical laboratory of functional diagnostics of MMA named after THEM. Sechenov.
As in the case of patients with US, preliminary examination in specialized institutions completely excluded cardiovascular and neurological pathology.
Patients presented persistent and numerous complaints of unpleasant and painful aching, oppressive or pulling character, localized in the region of the heart.
In medicine, there are several schemes for explaining functional pain in the region of the heart. The neurological concept links them to secondary radicular pains in case of cervical osteo-chondrosis, a lesion of a cervical stellate node or intercostal neuralgia (Popelyansky, 1989).
From the point of view of the biochemical concept, cardialgia occurs in the framework of neurocirculatory dystonia as a consequence of adrenal cardiomyopathy, hyperlactaemia, or increased catecholamine secretion.
The most common presentation is based on cortico-visceral theory, considering heart pain as a result of systemic psychogenic visceral disorders, the formation of a vicious cycle of stimulation of vegetative heart devices and sustained dominant arousal in the CNS {Karvasarsky, 1980; Topolyansky, Strukovskaya, 1986).
All these explanations are to a certain extent speculative and the mechanism of symptom formation of cardialgia remains rather unclear, but, just as in the case of the abdominal syndrome, the main efforts of researchers are aimed at finding a material substrate at the cellular or biochemical level.
The comparison group included 12 people with cholelithiasis (ICD), calculous cholecystitis. Disease duration from 0.5 to 12 years. Patients had a pain syndrome of organic nature (the presence of a stone in the gallbladder, verified by ultrasound tomography, and later on surgery). Intraceptive sensations were localized, as a rule, in the region of the right hypochondrium, at the point of the gallbladder, were irradiated in the back, sometimes were of a shingles character. By character - cutting, stabbing, bursting.
Patients with gallstone disease were on a hundred
inpatient treatment at the faculty surgical clinic MMA
them. IM Sechenov. *
As a control group , healthy subjects were examined (25 people). The principle of selection in the control group was the absence of any chronic or acute diseases at the time of the survey.
8.4. Research methods
With the subjects was conducted a study of the placebo effect in three variants.
Placebo capsule. The experiment was conducted in two stages. At the first stage, the subject was given a capsule filled with an inert substance under “deaf” instructions: “A substance is located in the capsule that affects the sensitivity of nerve endings. Some time after taking the capsule, sensations may appear in your body. Report any sensations immediately to the experimenter. ” After that within 20-30 minutes. all arising sensations, the time of their appearance, character, intensity, sequence were recorded.
At the second stage, the subject was given an "open" instruction - it was reported that "now should appear" certain sensations in a particular organ. Attention was consistently recorded on the limbs, abdomen, heart, and head.
Плацебо-электрод. В обстановке электроэнцефалографического кабинета на голову испытуемого одевалась специальная шапочка с электродами и говорилось, что на электроды будут подаваться «слабые сигналы». В дальнейшем проводилось два этапа: с «глухой» и «открытой» инструкциями, аналогичными инструкциям в экспе риментах с плацебо-капсулой.
Ложная биологическая обратная связь. В ситуации «плацебо-электрод» перед испытуемым устанавливалась мигающая лампочка и объяснялось, что частота мигания «соответствует интенсивности сигнала, подаваемого на электрод». Предлагалось отметить появле ние и исчезновение ощущения пульсации в голове. После этого 3 раза менялась частота мигания лампочки от 0,5 до 30 Гц и отмеча лось число совпадений учащения мигания лампочки с появлением и исчезновением ощущений. Интенсивность эффекта оценивалась в рангах:
• — ни разу не возникает ощущения пульсации;
• — возникает в 1 пробе из 3;
• — в 2 пробах из 3;
• — в 3 пробах из 3.
8.5. Обсуждение результатов
Наиболее интересный результат заключается в том, что величина плацебо-эффекта оказалась значительно выше, чем это обыч но предполагалось. Единственный сопоставимый результат — это частота плацебо-эффекта у здоровых испытуемых (52 %).
|
|
|
|
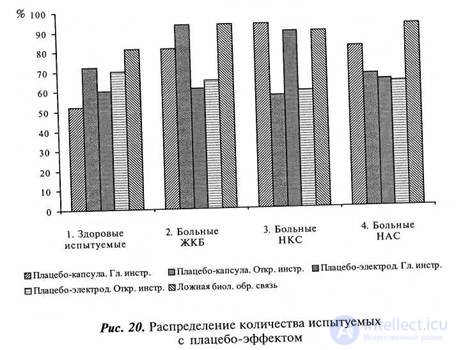
На рисунке 20 представлена диаграмма распределения количества испытуемых (%), у которых отмечалось появление интрацептивных ощущений в условиях «глухой» и «открытой» инструкций в эк спериментах «плацебо-капсула», «плацебо-электрод» и «ложной обратной связи».
Как можно видеть, в условиях «глухой» инструкции высокая частота плацебо-эффекта отмечается как у больных реальными за болеваниями (ЖКБ), так и у больных с функциональными абдоминалгическим и кардиалгическим синдромами. Значимо ниже (р<0,05) величина плацебо-эффекта у здоровых испытуемых. Это позволяет предполагать, что необходимым условием его формиро вания является развитая система языка тела — набора знакомых, усвоенных телесных ощущений, в которых только и может реализоваться плацебо-эффект.
При этом, хотя больные реальными и функциональными заболеваниями показывают количественно сходные результаты, содержательно структура возникающих ощущений очень различается.
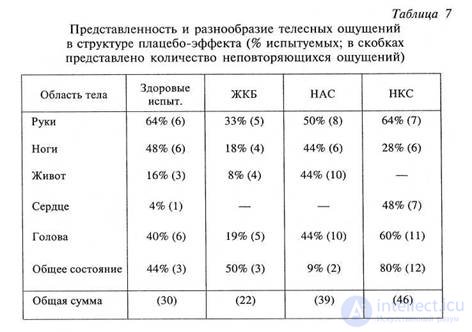
У здоровых испытуемых и больных ЖКБ появляются хорошо знакомые из обыденного опыта ощущения онемения, тяжести, хо лода и теплоты, локализованные преимущественно в конечностях. У больных с абдоминалгическим и кардиалгическим синдромом после приема плацебо разворачивается (полностью или фрагмен тарно) специфический болезненный приступ в той же последо вательности, в какой он обычно и происходит. Более 90 % возни кающих ощущений знакомы больным по опыту своей болезни. Интересна и закономерность локализации, четко отражающая степень объективированности и освоенности областей тела. В таблице 7 представлено процентное распределение числа испытуемых по раз нообразию и локализации возникающих ощущений (в скобках — количество неповторяющихся ощущений).
The sensations that appear in healthy subjects are quite monotonous and appear in well-developed areas of the body. The average number of sensations is small and amounts to 2.9 ± 0.6. Diversity (the total amount of non-repeating sensations - an analogue of the volume of the dictionary) is 30.
Patients with gallstone disease demonstrate even poorer than normal vocabulary, stereotypically reproducing only
well-learned in everyday experience sensations. They almost never experience sensations from the repertoire of a real painful attack, and the number of sensations in the abdomen is even less than in healthy subjects. The average number of sensations that occur after taking placebo is 2.2 ± 0.8,
variety - 22.
Совершенно иная картина у больных с функциональными алгическими синдромами. Основное количество возникающих ощуще ний (у больных НАС — 4,5 ± 0,9; у больных НКС — 4,9 ± 1) локализуется в области проявления болезни, причем словарь этих ощущений значимо увеличивается (разнообразие — 39 и 46). Инте ресны в этом смысле «общие изменения состояния организма». У больных НАС они достаточно редко включаются в картину прис тупа и столь же редко (в 9 % случаев) возникают в плацебо- эксперименте, тогда как у больных НКС они составляют практи чески обязательное сопровождение приступа и столь же часто (80 %) возникают в экспериментальной ситуации.
|
|
Изменение условий проведения эксперимента — переход к открытой инструкции — усиливает проявление плацебо-эффекта у здоровых испытуемых и больных ЖКБ и уменьшает у больных НАС и НКС (особенно у последних). В первых двух группах количество испытуемых, у которых появляются интрацептивные ощущения, увеличивается, а в двух последних уменьшается. Это очень важное обстоятельство позволяет оценить роль освоенного «сценария», раз ворачивающегося в ситуации плацебо-эксперимента. У здоровых ис пытуемых такого разработанного «сценария», как правило, нет и поэтому внешние опоры в виде формулировок, даваемых экспериментатором, облегчают формирование телесных ощущений, тогда как у больных с функциональными алгическими расстройствами они лишь мешают проявлению хорошо освоенного индивидуального паттерна. Иначе говоря, в условиях разработанного и хорошо освоенного стереотипа внешние инструкции, если они не вписывают ся в него, лишь мешают, а в случае же отсутствия такого стереотипа — предоставляют испытуемому необходимый язык. У больных ЖКБ объем ощущений в условиях открытой инструкции, так же как и у здоровых испытуемых, увеличивается. Объяснение заключается в том, что хотя болезненные ощущения им хорошо известны, но име ют совершенно иную природу и основываются на объективных при чинах, а мифологический способ их порождения и больными и здоровыми испытуемыми освоен в равной степени недостаточно.
Аналогичные тенденции сохраняются в эксперименте «плацебо- электрод», правда, с некоторыми интересными особенностями (см. рис. 20). Эффект «плацебо-электрода» в сравнении с «плацебо-капсулой» несколько увеличивается у здоровых испытуемых и значимо уменьшается у больных ЖКБ и НАС. Можно предположить, что капсула, принимаемая внутрь, имеет большую семантическую связь с типичными для этих больных ощущениями в области живота, чем электрод на голове. Высокая же эффективность электрода у здоровых испытуемых и у больных НКС предположительно можно свя зать с тем, что и в том и в другом случае ведущую роль в структуре плацебо-эффекта играют ощущения в области головы и ощущения общего тонуса, имеющие достаточно понятную смысловую связь с «влиянием на мозг».
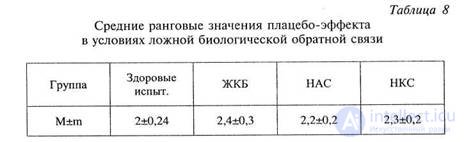
Введение дополнительного опосредствования через создание ложной обратной связи значительно усиливает эффективность «пла цебо-электрода» во всех группах испытуемых. Хотя можно отметить большую выраженность этого эффекта у больных ЖКБ и НКС, эти различия в ранговых значениях не существенны. Внешнее опосредствование становится главным фактором, нивелирующим влия ние других переменных (табл. 8).
Косвенный результат экспериментов с ложной биологической обратной связью заставляет переосмыслить многие результаты, по лученные в обширной области « bio - feedback », часть из которых, возможно, представляет собой не что иное, как «наведенный» пла цебо-эффект.
Что же касается нашей проблемы, то, обобщая предваритель ные результаты, можно сделать следующие, пока самые общие вы воды.
Во-первых, мы получили прямое экспериментальное доказа тельство принципиальной возможности порождения конкретных те лесных ощущений через се миологическую конструкцию мифа. Это подтверждает наше теоретическое положение о том, что субъек тивное существование интрацептивного ощущения может в значительной степени расходиться с реальными телесными событиями, отражением которых оно должно было быть, если исходить из представлений о его рефлекторном характере. Величина плацебо эффекта, полученная в экспериментах, показывает, что роль семиологической составляющей лечебного процесса весьма велика и в некоторых случаях может обеспечивать более 90 % непосредствен ного субъективного эффекта.
Во-вторых, сам плацебо-эффект следует рассматривать как сложный феномен семиологической конструкции лечебного воздей ствия, величина которого может быть значительно изменена спосо бом его включения в эту конструкцию.
В-третьих, уровень и эффективность семиологического опосред ствования телесных ощущений увеличены у больных с функцио нальными алгическими синдромами и, по-видимому, принимают непосредственное участие в симптомообразовании. Хотя сам по себе этот факт еще не объясняет патогенетического механизма таких рас стройств, можно довольно уверенно утверждать, что длительный спор, ведущийся по поводу поисков резидуальных органических нарушений при функциональных алгических синдромах, в зна чительной мере искусственен. То, что весь набор интрацептивных ощущений, входящий в жалобы этих больных, может быть вызван знаковым раздражителем, свидетельствует о том, что если даже по добные нарушения и могут быть найдены, они играют отнюдь не главную роль и не объясняют формирования симптома. Значительно более важны психологические параметры, на изучение которых и следует сместить исследовательский акцент. Хотя семиотическое по рождение телесных ощущений — вполне нормальный процесс, оно в силу каких-то еще не ясных для нас обстоятельств может приоб ретать патологический характер и плохо коррегироваться реальнос тью. Необходимо выяснить, почему в одних случаях интрацептивные ощущения, не имеющие под собой реальной почвы, носят транзиторный ситуационный характер, а в других — фиксируются в виде патологических синдромов; определить, что приводит к их стабилизации, чем определяется эффективность семиологического опосредствования интрацепции и какими психологическими или психофизиологическими механизмами оно обеспечивается. Попыт кам ответить на эти вопросы посвящены два следующих блока наших экспериментов.


Comments
To leave a comment
The psychology of corporeality
Terms: The psychology of corporeality